

The immune response to SARS-CoV-2 in people with HIV
- PMID: 37821620
- PMCID: PMC10806256
- DOI: 10.1038/s41423-023-01087-w
The immune response to SARS-CoV-2 in people with HIV
Abstract
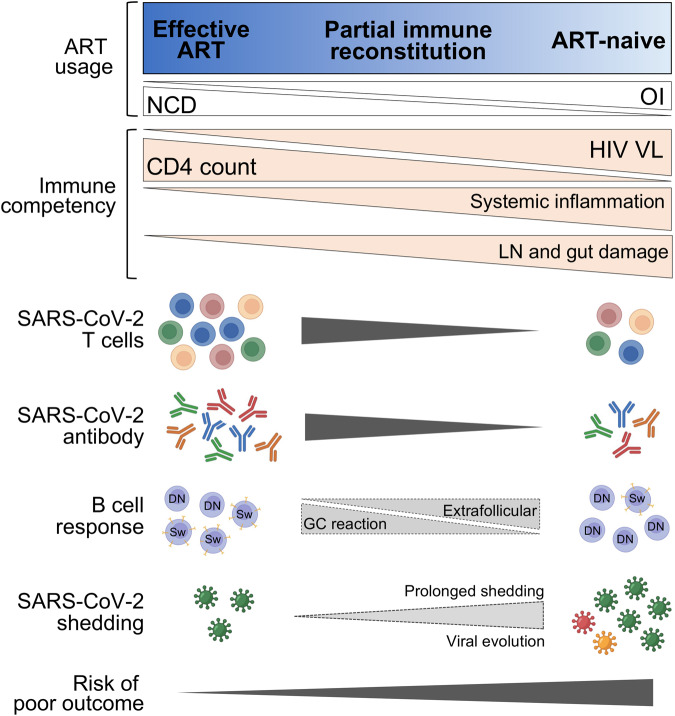
This review examines the intersection of the HIV and SARS-CoV-2 pandemics. People with HIV (PWH) are a heterogeneous group that differ in their degree of immune suppression, immune reconstitution, and viral control. While COVID-19 in those with well-controlled HIV infection poses no greater risk than that for HIV-uninfected individuals, people with advanced HIV disease are more vulnerable to poor COVID-19 outcomes. COVID-19 vaccines are effective and well tolerated in the majority of PWH, though reduced vaccine efficacy, breakthrough infections and faster waning of vaccine effectiveness have been demonstrated in PWH. This is likely a result of suboptimal humoral and cellular immune responses after vaccination. People with advanced HIV may also experience prolonged infection that may give rise to new epidemiologically significant variants, but initiation or resumption of antiretroviral therapy (ART) can effectively clear persistent infection. COVID-19 vaccine guidelines reflect these increased risks and recommend prioritization for vaccination and additional booster doses for PWH who are moderately to severely immunocompromised. We recommend continued research and monitoring of PWH with SARS-CoV-2 infection, especially in areas with a high HIV burden.
Keywords: HIV; Immune dysfunction; Immunogenicity; Prolonged infection; SARS-CoV-2; Vaccine efficacy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Harboe ZB, Larsen MV, Ladelund S, Kronborg G, Konradsen HB, Gerstoft J, et al. Incidence and risk factors for invasive pneumococcal disease in HIV-infected and non-HIV-infected individuals before and after the introduction of combination antiretroviral therapy: persistent high risk among HIV-infected injecting drug users. Clin Infect Dis. 2014;59:1168–76. doi: 10.1093/cid/ciu558. - DOI - PubMed
-
- Gazzola L, Tincati C, Bellistri GM, Monforte A, Marchetti G. The absence of CD4+ T cell count recovery despite receipt of virologically suppressive highly active antiretroviral therapy: clinical risk, immunological gaps, and therapeutic options. Clin Infect Dis. 2009;48:328–37. doi: 10.1086/695852. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
