

Redefining serological diagnostics with immunoaffinity proteomics
- PMID: 37821808
- PMCID: PMC10568870
- DOI: 10.1186/s12014-023-09431-y
Redefining serological diagnostics with immunoaffinity proteomics
Abstract
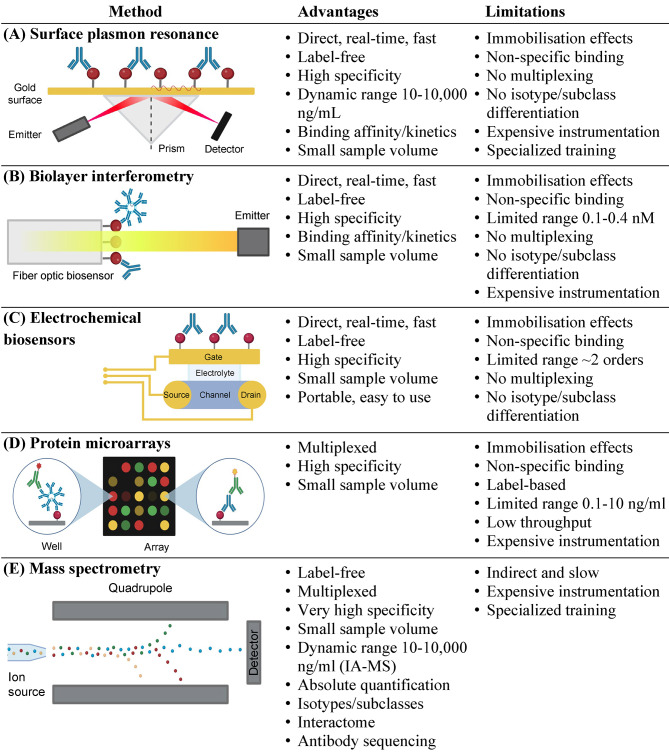
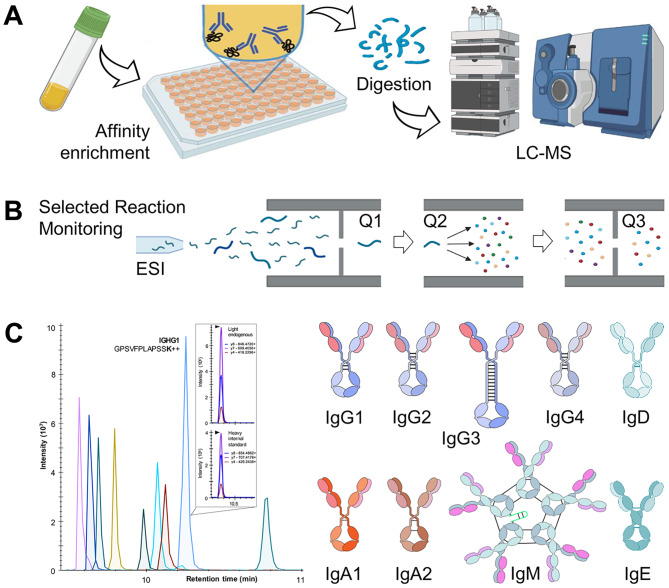
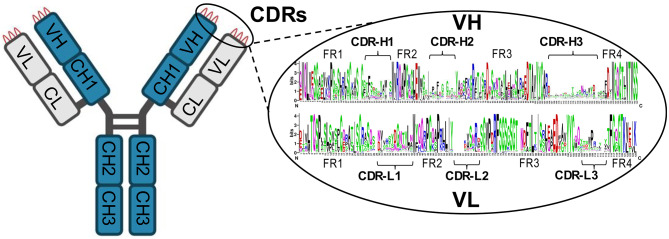
Serological diagnostics is generally defined as the detection of specific human immunoglobulins developed against viral, bacterial, or parasitic diseases. Serological tests facilitate the detection of past infections, evaluate immune status, and provide prognostic information. Serological assays were traditionally implemented as indirect immunoassays, and their design has not changed for decades. The advantages of straightforward setup and manufacturing, analytical sensitivity and specificity, affordability, and high-throughput measurements were accompanied by limitations such as semi-quantitative measurements, lack of universal reference standards, potential cross-reactivity, and challenges with multiplexing the complete panel of human immunoglobulin isotypes and subclasses. Redesign of conventional serological tests to include multiplex quantification of immunoglobulin isotypes and subclasses, utilize universal reference standards, and minimize cross-reactivity and non-specific binding will facilitate the development of assays with higher diagnostic specificity. Improved serological assays with higher diagnostic specificity will enable screenings of asymptomatic populations and may provide earlier detection of infectious diseases, autoimmune disorders, and cancer. In this review, we present the major clinical needs for serological diagnostics, overview conventional immunoassay detection techniques, present the emerging immunoassay detection technologies, and discuss in detail the advantages and limitations of mass spectrometry and immunoaffinity proteomics for serological diagnostics. Finally, we explore the design of novel immunoaffinity-proteomic assays to evaluate cell-mediated immunity and advance the sequencing of clinically relevant immunoglobulins.
Keywords: Immunoassays.; Immunoglobulins; Mass spectrometry; Proteomics; Serological diagnostics.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Rational Design and Development of SARS-CoV-2 Serological Diagnostics by Immunoprecipitation-Targeted Proteomics.Anal Chem. 2022 Sep 27;94(38):12990-12999. doi: 10.1021/acs.analchem.2c01325. Epub 2022 Sep 12. Anal Chem. 2022. PMID: 36095284 Free PMC article.
-
Mass spectrometry-based proteomics in basic and translational research of SARS-CoV-2 coronavirus and its emerging mutants.Clin Proteomics. 2021 Aug 12;18(1):19. doi: 10.1186/s12014-021-09325-x. Clin Proteomics. 2021. PMID: 34384361 Free PMC article. Review.
-
Emerging Affinity-Based Proteomic Technologies for Large-Scale Plasma Profiling in Cardiovascular Disease.Circulation. 2017 Apr 25;135(17):1651-1664. doi: 10.1161/CIRCULATIONAHA.116.025446. Circulation. 2017. PMID: 28438806 Free PMC article. Review.
-
Conjugating immunoassays to mass spectrometry: Solutions to contemporary challenges in clinical diagnostics.Trends Analyt Chem. 2020 Nov;132:116064. doi: 10.1016/j.trac.2020.116064. Epub 2020 Oct 7. Trends Analyt Chem. 2020. PMID: 33046944 Free PMC article. Review.
-
How to interpret and use COVID-19 serology and immunology tests.Clin Microbiol Infect. 2021 Jul;27(7):981-986. doi: 10.1016/j.cmi.2021.05.001. Epub 2021 May 8. Clin Microbiol Infect. 2021. PMID: 33975005 Free PMC article. Review.
Cited by
-
A Careful Insight into DDI-Type Receptor Layers on the Way to Improvement of Click-Biology-Based Immunosensors.Biosensors (Basel). 2024 Mar 6;14(3):136. doi: 10.3390/bios14030136. Biosensors (Basel). 2024. PMID: 38534243 Free PMC article.
References
-
- Wassermann, Av Bruck CGv. Experimentelle Studien über die Wirkung von Tuberkelbacillen-Präparaten auf den tuberculös erkrankten Organismus. Dtsch Med Wochenschr. 1906;32:449–54.
-
- Allard-Chamard H, Boire G. Serologic diagnosis of rheumatoid arthritis. Clin Lab Med. 2019;39(4):525–37. - PubMed
-
- Lindfors K, Ciacci C, Kurppa K, Lundin KEA, Makharia GK, Mearin ML, et al. Coeliac disease. Nat Reviews Disease Primers. 2019;5(1):3. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous