

Severe Pediatric COVID-19 and Multisystem Inflammatory Syndrome in Children From Wild-type to Population Immunity: A Prospective Multicenter Cohort Study With Real-time Reporting
- PMID: 37823702
- PMCID: PMC10629607
- DOI: 10.1097/INF.0000000000004098
Severe Pediatric COVID-19 and Multisystem Inflammatory Syndrome in Children From Wild-type to Population Immunity: A Prospective Multicenter Cohort Study With Real-time Reporting
Abstract
Background: SARS-CoV-2 variant evolution and increasing immunity altered the impact of pediatric SARS-CoV-2 infection. Public health decision-making relies on accurate and timely reporting of clinical data.
Methods: This international hospital-based multicenter, prospective cohort study with real-time reporting was active from March 2020 to December 2022. We evaluated longitudinal incident rates and risk factors for disease severity.
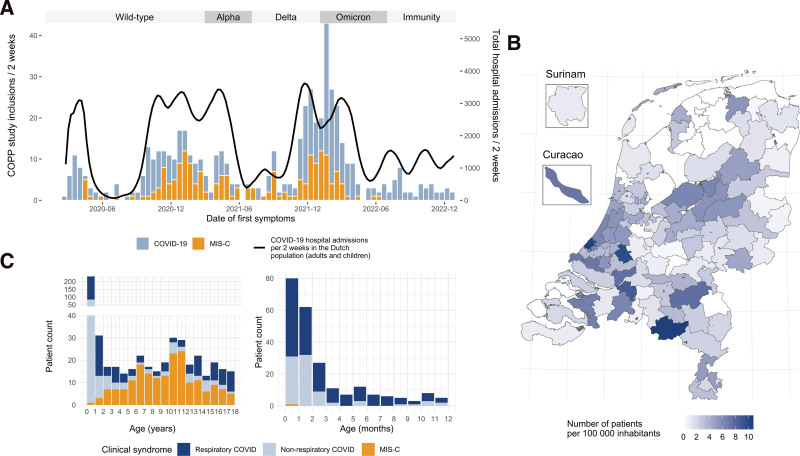
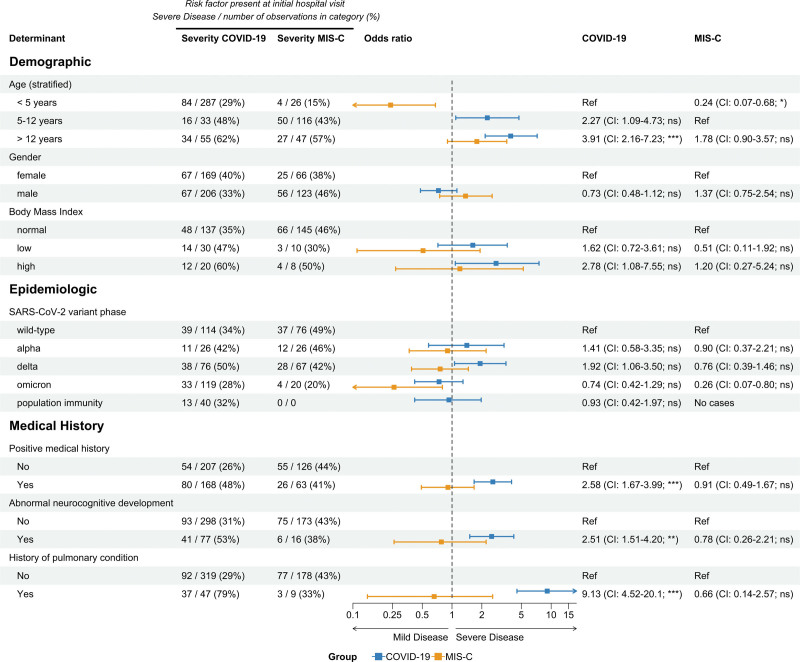
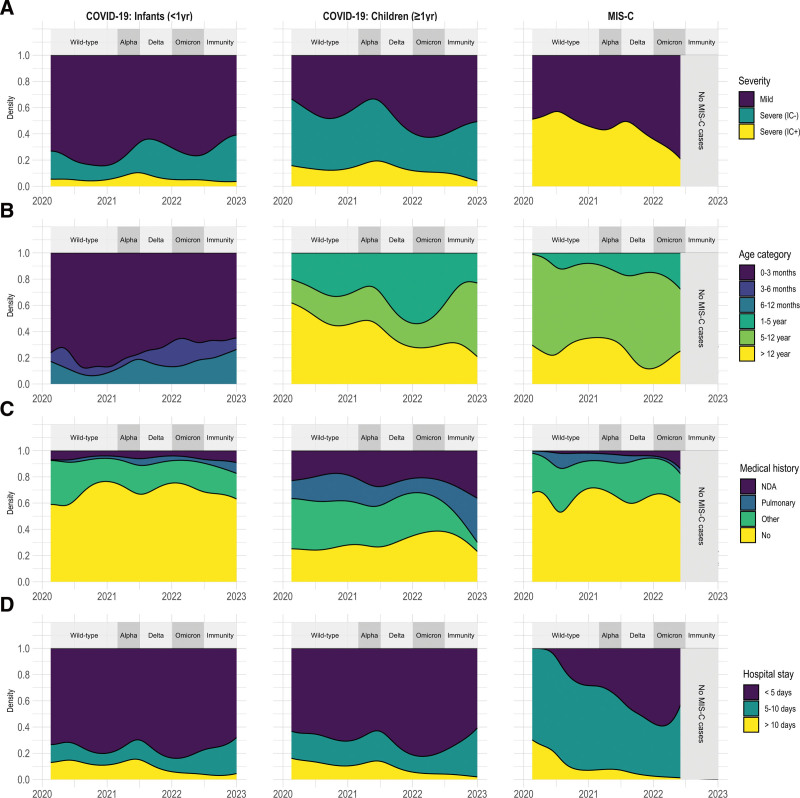
Results: We included 564 hospitalized children with acute COVID-19 (n = 375) or multisystem inflammatory syndrome in children (n = 189) from the Netherlands, Curaçao and Surinam. In COVID-19, 134/375 patients (36%) needed supplemental oxygen therapy and 35 (9.3%) required intensive care treatment. Age above 12 years and preexisting pulmonary conditions were predictors for severe COVID-19. During omicron, hospitalized children had milder disease. During population immunity, the incidence rate of pediatric COVID-19 infection declined for older children but was stable for children below 1 year. The incidence rate of multisystem inflammatory syndrome in children was highest during the delta wave and has decreased rapidly since omicron emerged. Real-time reporting of our data impacted national pediatric SARS-CoV-2 vaccination- and booster-policies.
Conclusions: Our data supports the notion that similar to adults, prior immunity protects against severe sequelae of SARS-CoV-2 infections in children. Real-time reporting of accurate and high-quality data is feasible and impacts clinical and public health decision-making. The reporting framework of our consortium is readily accessible for future SARS-CoV-2 waves and other emerging infections.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Graff K, Smith C, Silveira L, et al. Risk factors for severe COVID-19 in children. Pediatr Infect Dis J. 2021;40:e137–e145. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
