

Challenging Clinical Perspectives in Type 2 Diabetes with Tirzepatide, a First-in-Class Twincretin
- PMID: 37824027
- PMCID: PMC10597955
- DOI: 10.1007/s13300-023-01475-5
Challenging Clinical Perspectives in Type 2 Diabetes with Tirzepatide, a First-in-Class Twincretin
Abstract
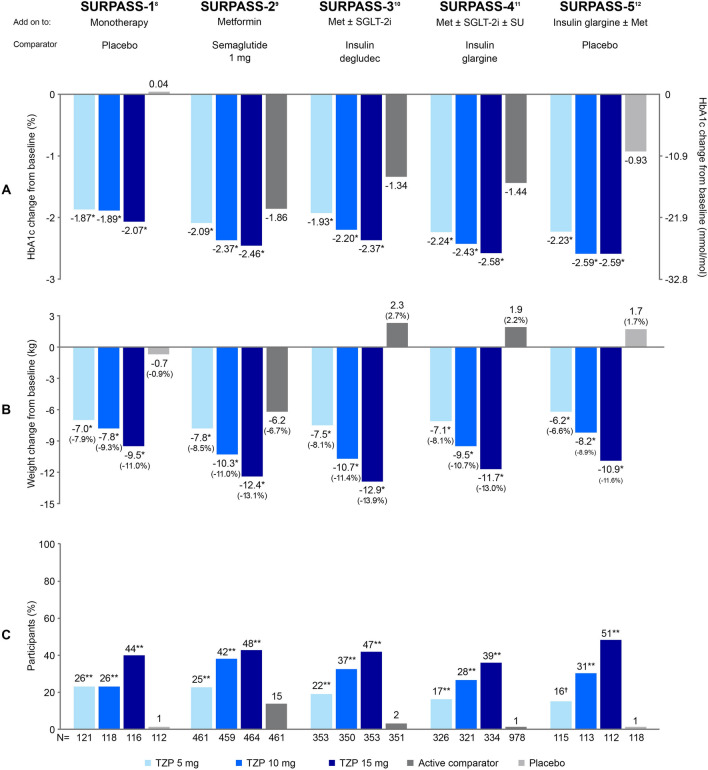
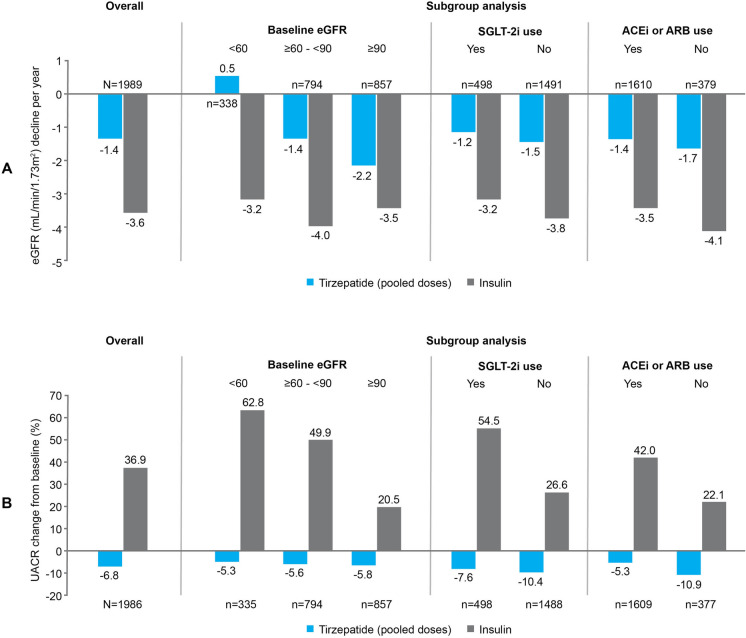
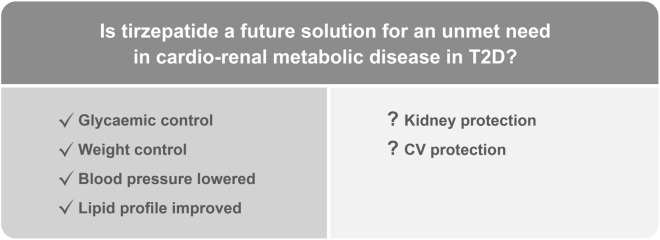
Tirzepatide is a first-in-class GIP/GLP-1 receptor agonist ('twincretin')-a single molecule that acts as an agonist at both glucagon-like peptide 1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) receptors. In the SURPASS clinical trial program in type 2 diabetes mellitus (T2D), tirzepatide was associated with unprecedented reductions in HbA1c, clinically significant weight loss and other metabolic benefits, combined with low rates of hypoglycaemia across a wide range of patient characteristics. The safety and adverse event rate for tirzepatide appears comparable to that of GLP-1 receptor agonists. Although results from dedicated cardiovascular (CV) and kidney trials are currently not available, information to date suggests that tirzepatide may have CV and kidney benefits in people with T2D. Tirzepatide has been approved for the treatment of T2D in the USA, United Arab Emirates, European Union, Japan and Australia. Here, we review how tirzepatide will fit into the T2D treatment continuum. We also consider future directions with tirzepatide in T2D, including its potential for targeting cardio-renal-metabolic disease in T2D, and discuss how tirzepatide-and other co-agonists in development-may challenge current approaches for management of T2D.
Keywords: Body weight/drug therapy; Cardio-renal-metabolic disease; GIP/GLP-1 receptor agonist; SURPASS clinical trials; Tirzepatide; Twincretin; Type 2 diabetes/drug therapy.
© 2023. The Author(s).
Conflict of interest statement
Richard MacIsaac: Has received research grants from Novo Nordisk, Servier, Medtronic, The Rebecca Cooper Medical Research Foundation, St Vincent’s Research Foundation, The Juvenile Diabetes Research Foundation, Grey Innovations, The Diabetes Australia Research Trust/Program and The National Health and Medical Research Council of Australia. Also received honoraria for lectures from Eli Lilly, Novo Nordisk, Sanofi Aventis, AstraZeneca, Merck Sharp & Dohme, Norvartis and Boehringer Ingelheim and has been or is on the advisory boards for Novo Nordisk, Boehringer Ingelheim-Eli Lilly Diabetes Alliance, AstraZeneca and Merck Shape and Dohme. Travel support has been supplied by Novo Nordisk, Sanofi, Boehringer Ingelheim and AstraZeneca. Has been a principal investigator for industry-sponsored clinical trials run by Novo Nordisk, Sanofi, Bayer, Johnson-Cilag and AbbVie. Gary Deed: Has provided Advisory Board consultancy to Eli Lilly regarding tirzepatide, has provided medical education consultancy or been on advisory boards for AstraZeneca, Boehringer Ingelheim, Eli Lilly Australia, MSD Australia, Novo Nordisk and Sanofi-Aventis Australia, and provides educational support in diabetes management. Michael D’Emden: Has received honoraria for attendance at national advisory boards, presentations and/or support to attend international meetings from Boehringer Ingelheim, Eli Lilly, AstraZeneca, Novartis, Abbott, Novo Nordisk, Servier and Bayer. Elif I. Ekinci: Has been a member of advisory boards for Eli Lilly, Sanofi, Pfizer, and Bayer; income received is donated to EE’s institution for diabetes research. Speakers fees for presentations for Eli Lilly, Bayer and Sanofi have been donated to EE’s institution for diabetes research. EE’s institution has received research funding from Eli Lilly, Boehringer, Sanofi, Novo Nordisk, Gilead and Insulet. Samantha Hocking: Has received research grants from Novo Nordisk, The Diabetes Australia Research Trust/Program and The National Health and Medical Research Council of Australia. Also received honoraria for lectures from Eli Lilly, Boehringer Ingelheim, Novo Nordisk, Sanofi Aventis, AstraZeneca, Gilead, Inova and Merck Sharp & Dohme and has been or is on the advisory boards for Novo Nordisk, Eli Lilly, AstraZeneca, Inova and Pfizer. Has been a principal investigator for industry-sponsored clinical trials run by Novo Nordisk, Eli Lilly, Boehringer Ingelheim and Merck Sharp & Dohme. Co-authorship of manuscripts assisted by medical writing from Novo Nordisk. Priya Sumithran: Has received research grants paid to the Institution from National Health and Medical Research Council. Co-authorship of manuscripts assisted by medical writing from Novo Nordisk. Roy Rasalam: Has provided medical education consultancy or been on advisory boards for AstraZeneca, Boehringer Ingelheim, Eli Lilly Australia, MSD Australia, Novo Nordisk and Sanofi-Aventis Australia.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
