Toll-Like Receptor 4 Agonist Injection With Concurrent Radiotherapy in Patients With Metastatic Soft Tissue Sarcoma: A Phase 1 Nonrandomized Controlled Trial
- PMID: 37824131
- PMCID: PMC10570919
- DOI: 10.1001/jamaoncol.2023.4015
Toll-Like Receptor 4 Agonist Injection With Concurrent Radiotherapy in Patients With Metastatic Soft Tissue Sarcoma: A Phase 1 Nonrandomized Controlled Trial
Abstract
Importance: Metastatic soft tissue sarcomas (STSs) have limited systemic therapy options, and immunomodulation has not yet meaningfully improved outcomes. Intratumoral (IT) injection of the toll-like receptor 4 (TLR4) agonist glycopyranosyl lipid A in stable-emulsion formulation (GLA-SE) has been studied as immunotherapy in other contexts.
Objective: To evaluate the safety, efficacy, and immunomodulatory effects of IT GLA-SE with concurrent radiotherapy in patients with metastatic STS with injectable lesions.
Design, setting, and participants: This phase 1 nonrandomized controlled trial of patients with STS was performed at a single academic sarcoma specialty center from November 17, 2014, to March 16, 2016. Data analysis was performed from August 2016 to September 2022.
Interventions: Two doses of IT GLA-SE (5 μg and 10 μg for 8 weekly doses) were tested for safety in combination with concurrent radiotherapy of the injected lesion.
Main outcomes and measures: Primary end points were safety and tolerability. Secondary and exploratory end points included local response rates as well as measurement of antitumor immunity with immunohistochemistry and T-cell receptor (TCR) sequencing of tumor-infiltrating and circulating lymphocytes.
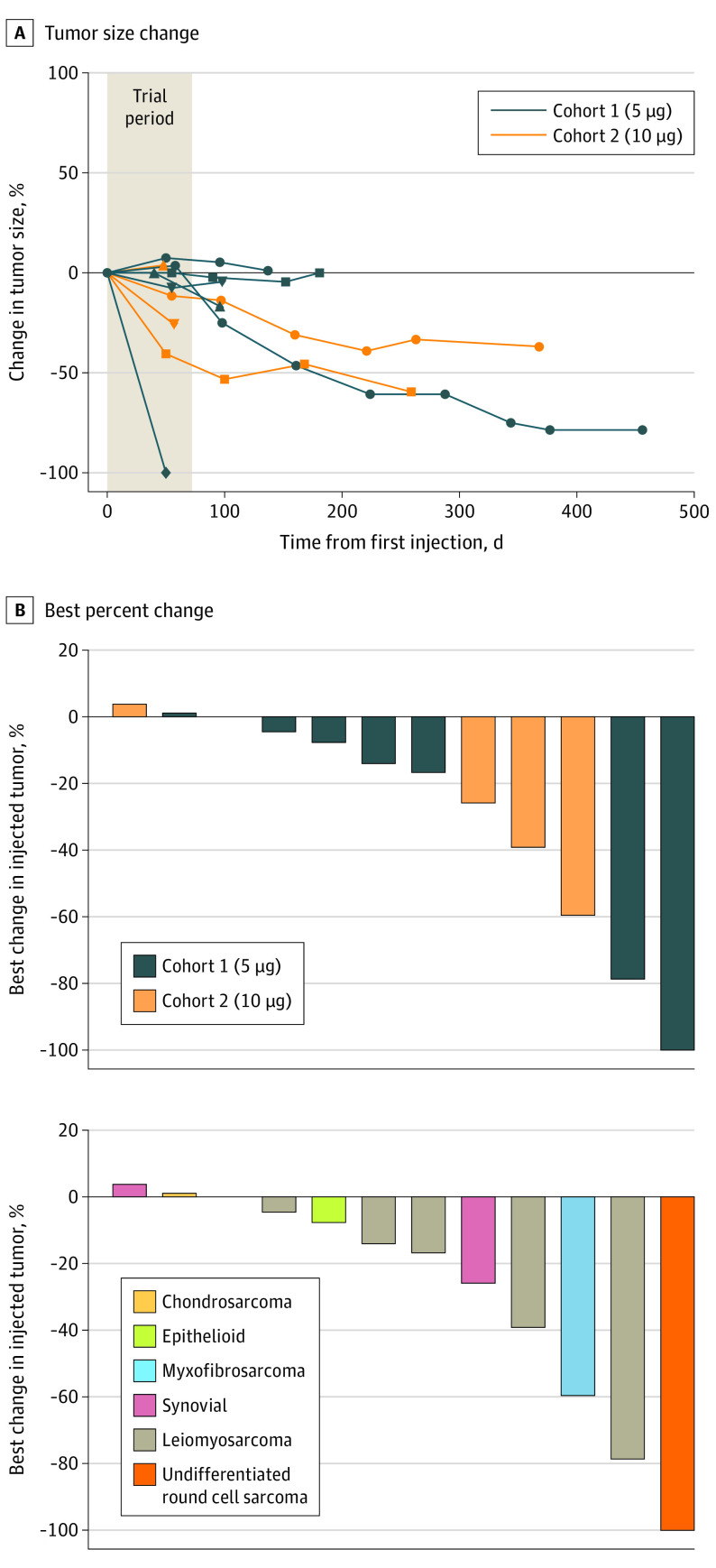
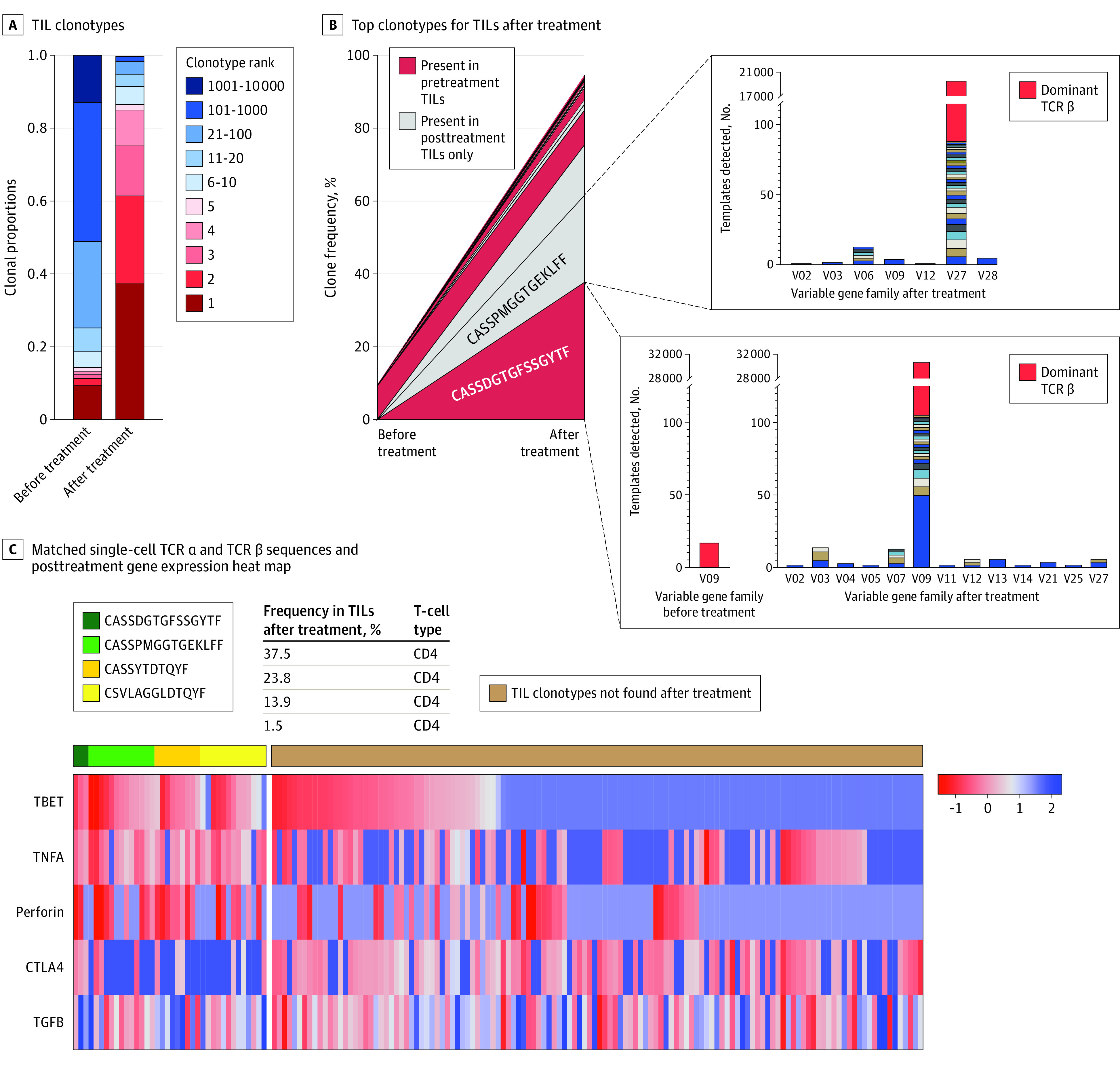
Results: Twelve patients (median [range] age, 65 [34-78] years; 8 [67%] female) were treated across the 2 dose cohorts. Intratumoral GLA-SE was well tolerated, with only 1 patient (8%) experiencing a grade 2 adverse event. All patients achieved local control of the injected lesion after 8 doses, with 1 patient having complete regression (mean regression, -25%; range, -100% to 4%). In patients with durable local response, there were detectable increases in tumor-infiltrating lymphocytes. In 1 patient (target lesion -39% at 259 days of follow-up), TCR sequencing revealed expansion of preexisting and de novo clonotypes, with convergence of numerous rearrangements coding for the same binding sequence (suggestive of clonal convergence to antitumor targets). Single-cell sequencing identified these same expanded TCR clones in peripheral blood after treatment; these T cells had markedly enhanced Tbet expression, suggesting TH1 phenotype.
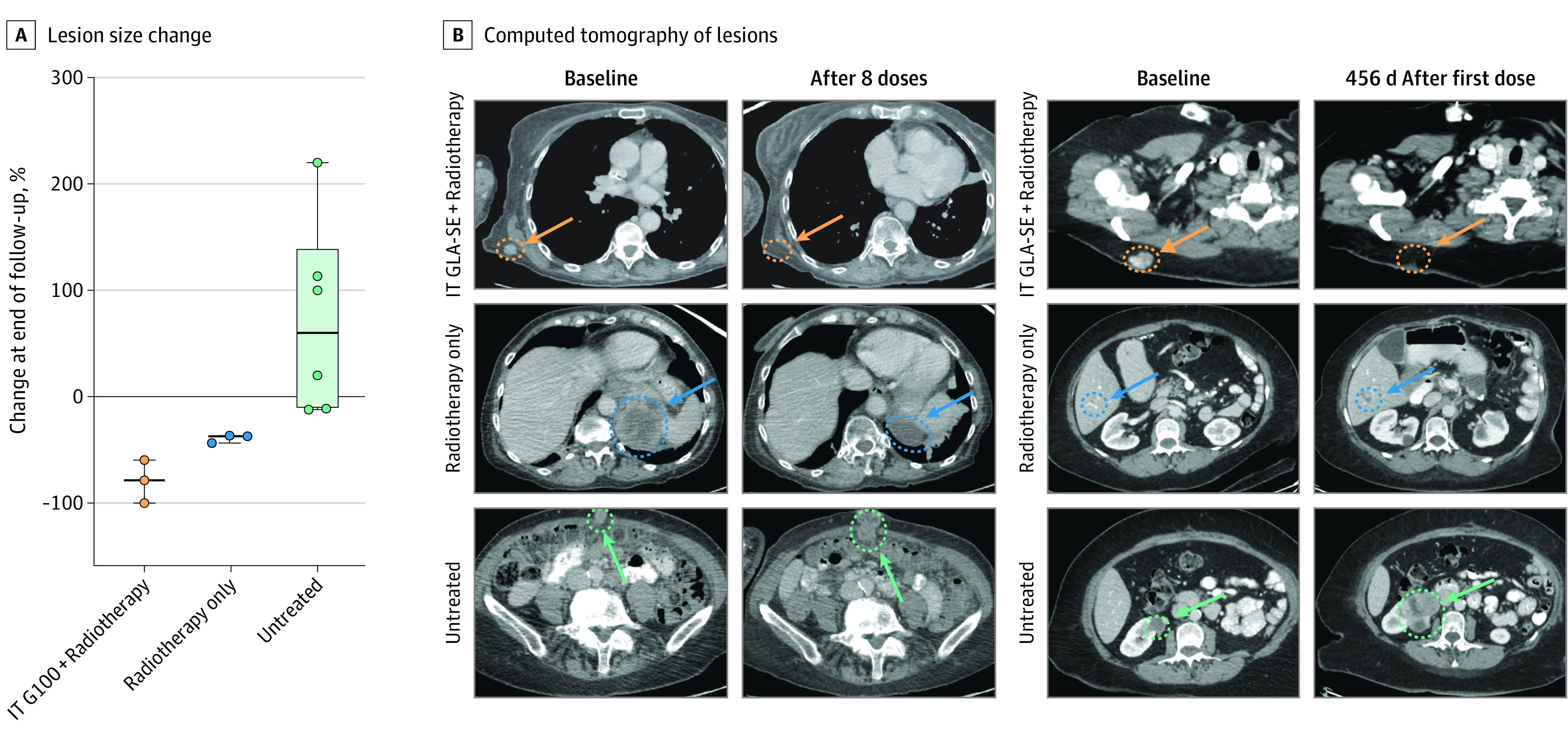
Conclusions and relevance: In this nonrandomized controlled trial, IT GLA-SE with concurrent radiotherapy was well tolerated and provided more durable local control than radiotherapy alone. Patients with durable local response demonstrated enhanced IT T-cell clonal expansion, with matched expansion of these clonotypes in the circulation. Additional studies evaluating synergism of IT GLA-SE and radiotherapy with systemic immune modulation are warranted.
Trial registration: ClinicalTrials.gov Identifier: NCT02180698.
Conflict of interest statement
Figures