

Cost-Effectiveness of Antiobesity Drugs for Adolescents With Severe Obesity
- PMID: 37824146
- PMCID: PMC10570871
- DOI: 10.1001/jamanetworkopen.2023.36400
Cost-Effectiveness of Antiobesity Drugs for Adolescents With Severe Obesity
Abstract
Importance: Although the American Academy of Pediatrics has recommended treatment with antiobesity drugs for adolescents, the cost-effectiveness of antiobesity drugs for this population is still unknown.
Objective: To quantify cost-effectiveness of different antiobesity drugs available for pediatric use.
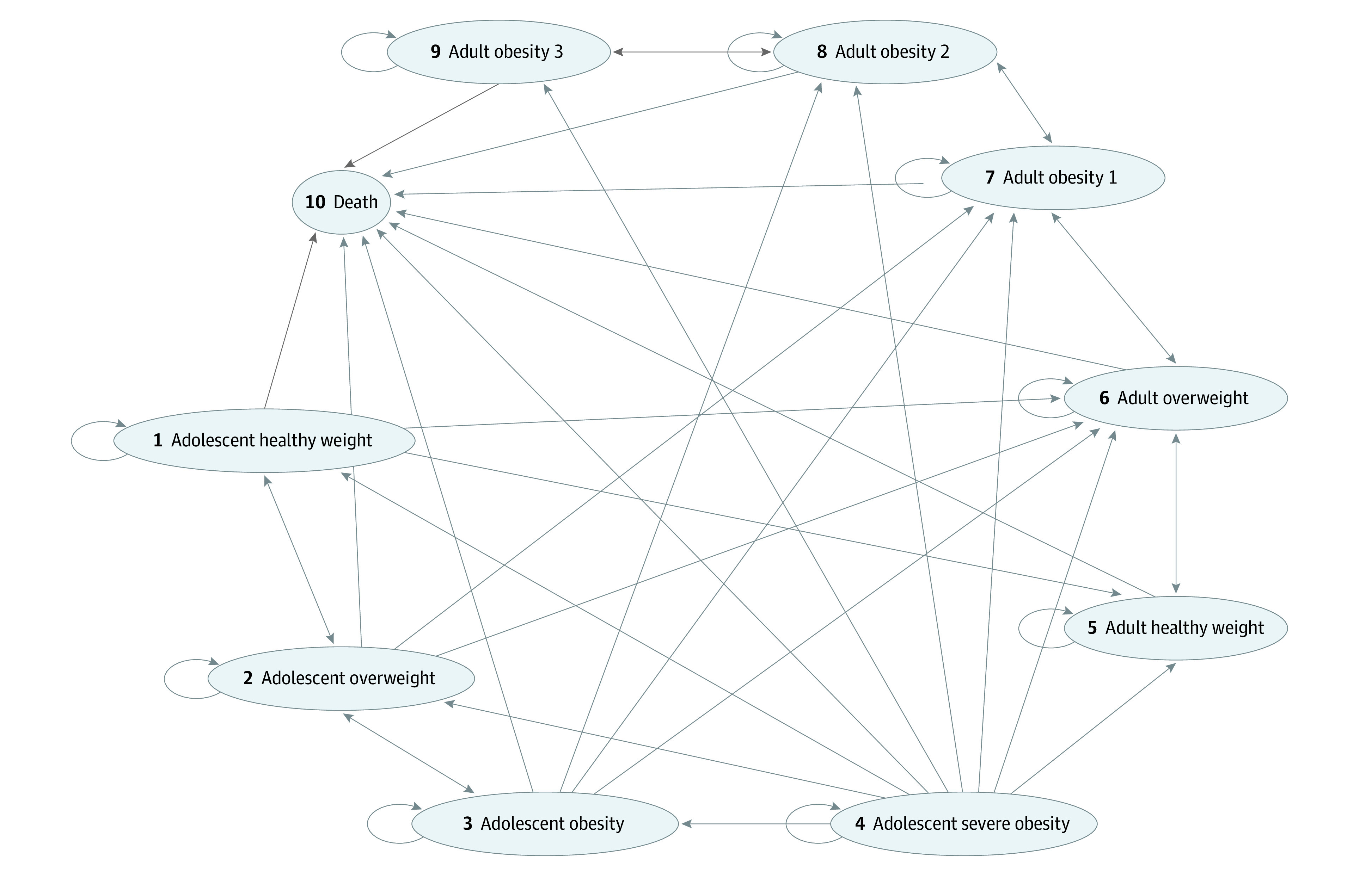
Design, setting, and participants: This economic evaluation used a Markov microsimulation model with health states defined by obesity levels. Effectiveness was measured by quality-adjusted life-years (QALYs) and costs were calculated from third-party payer perspective, estimated in 2023 US dollars over a 10-year horizon. Data were obtained from the published literature.
Intervention: Antiobesity drugs orlistat, liraglutide, semaglutide, and phentermine-topiramate vs no treatment. Metformin hydrochloride and 2 types of bariatric surgical procedures (sleeve gastrectomy and gastric bypass) were considered in sensitivity analysis.
Main outcomes and measures: Incremental cost-effectiveness ratio.
Results: Among the 4 antiobesity drugs currently approved for pediatric use, phentermine-topiramate was the most cost-effective with an incremental cost-effectiveness ratio of $93 620 per QALY relative to no treatment in this simulated cohort of 10 000 adolescents aged 12 to 17 years (mode, 15 years) with severe obesity (62% female). While semaglutide offered more QALYs than phentermine-topiramate, its higher cost resulted in an incremental cost-effectiveness ratio ($1 079 480/QALY) that exceeded the commonly used willingness-to-pay threshold of $100 000 to $150 000/QALY. Orlistat and liraglutide cost more and were less effective than phentermine-topiramate and semaglutide, respectively. Sleeve gastrectomy and gastric bypass were more effective than phentermine-topiramate but were also more costly, rendering them not cost-effective compared with phentermine-topiramate at the willingness-to-pay threshold of $100 000 to $150 000/QALY.
Conclusions and relevance: In this economic evaluation of weight loss drugs for adolescents with severe obesity, we found phentermine-topiramate to be a cost-effective treatment at a willingness-to-pay threshold of $100 000 to $150 000/QALY. Further research is needed to determine long-term drug efficacy and how long adolescents continue treatment.
Conflict of interest statement
Figures

Comment in
-
The Economic Value of Treating Pediatric Obesity: Costs Are Not Keeping Up With Efficacy.JAMA Netw Open. 2023 Oct 2;6(10):e2336337. doi: 10.1001/jamanetworkopen.2023.36337. JAMA Netw Open. 2023. PMID: 37824149 No abstract available.
References
-
- Reuters . US experts recommend weight-loss drugs for obese children. Published January 9, 2023. Accessed April 8, 2023. https://www.reuters.com/world/us/us-experts-recommend-weight-loss-drugs-...
-
- CBC News . Will Canada follow the US’s aggressive new approach to treat childhood obesity? Published February 14, 2023. Accessed April 8, 2023. https://www.cbc.ca/news/health/us-canada-obesity-guidelines-1.6746380
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
