

Pragmatic solutions to reduce the global burden of stroke: a World Stroke Organization-Lancet Neurology Commission
- PMID: 37827183
- PMCID: PMC10715732
- DOI: 10.1016/S1474-4422(23)00277-6
Pragmatic solutions to reduce the global burden of stroke: a World Stroke Organization-Lancet Neurology Commission
Erratum in
-
Correction to Lancet Neurol 2023; 22: 1160-206.Lancet Neurol. 2023 Dec;22(12):e13. doi: 10.1016/S1474-4422(23)00425-8. Lancet Neurol. 2023. PMID: 37977715 No abstract available.
Abstract
Stroke is the second leading cause of death worldwide. The burden of disability after a stroke is also large, and is increasing at a faster pace in low-income and middle-income countries than in high-income countries. Alarmingly, the incidence of stroke is increasing in young and middle-aged people (ie, age <55 years) globally. Should these trends continue, Sustainable Development Goal 3.4 (reducing the burden of stroke as part of the general target to reduce the burden of non-communicable diseases by a third by 2030) will not be met.
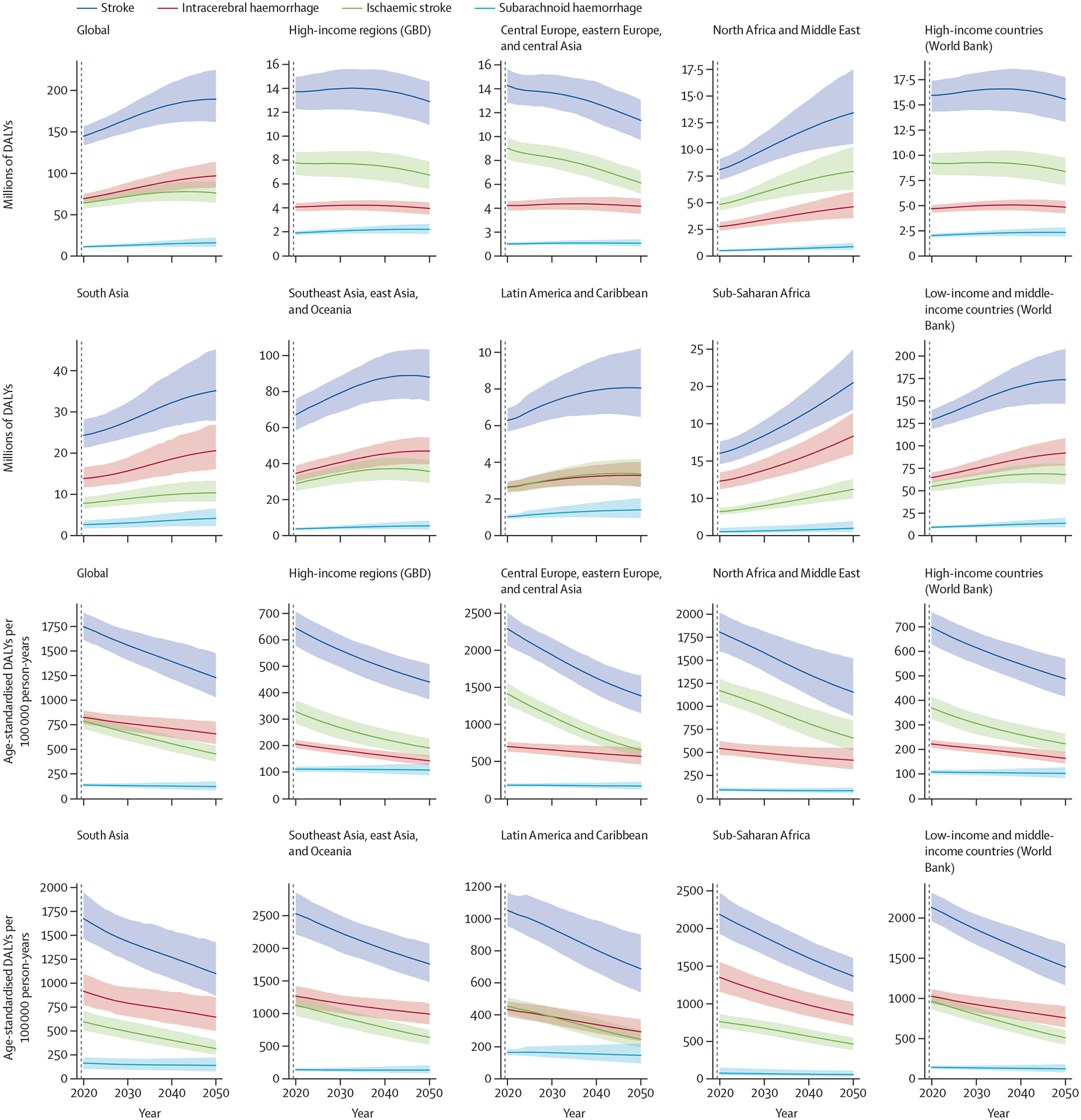
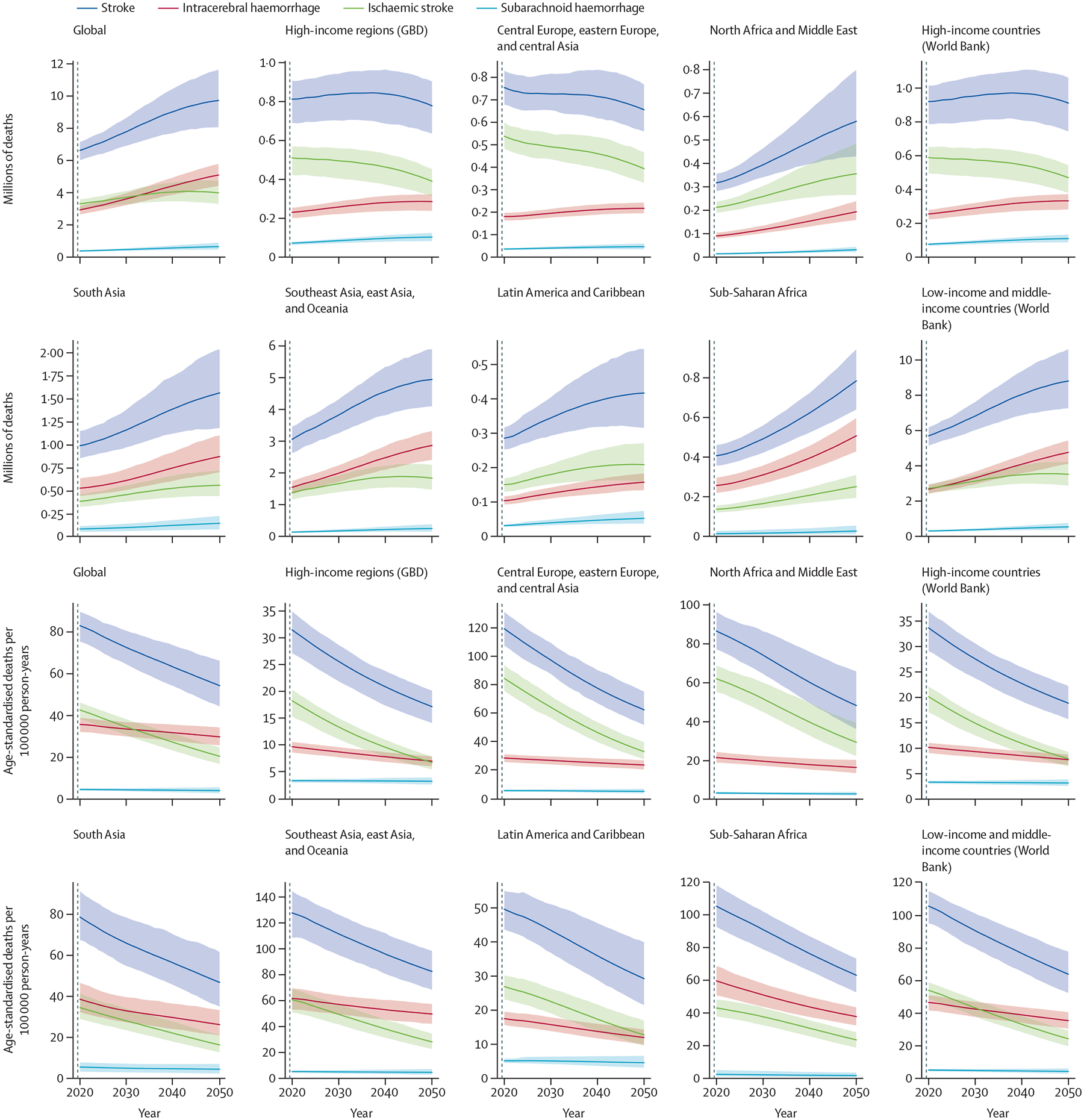
In this Commission, we forecast the burden of stroke from 2020 to 2050. We project that stroke mortality will increase by 50%—from 6·6 million (95% uncertainty interval [UI] 6·0 million–7·1 million) in 2020, to 9·7 million (8·0 million–11·6 million) in 2050—with disability-adjusted life-years (DALYs) growing over the same period from 144·8 million (133·9 million–156·9 million) in 2020, to 189·3 million (161·8 million–224·9 million) in 2050. These projections prompted us to do a situational analysis across the four pillars of the stroke quadrangle: surveillance, prevention, acute care, and rehabilitation. We have also identified the barriers to, and facilitators for, the achievement of these four pillars. The sum of the years of life lost as a result of premature mortality from a disease and the years lived with a disability associated with prevalent cases of the disease in a population. One DALY represents the loss of the equivalent of one year of full health
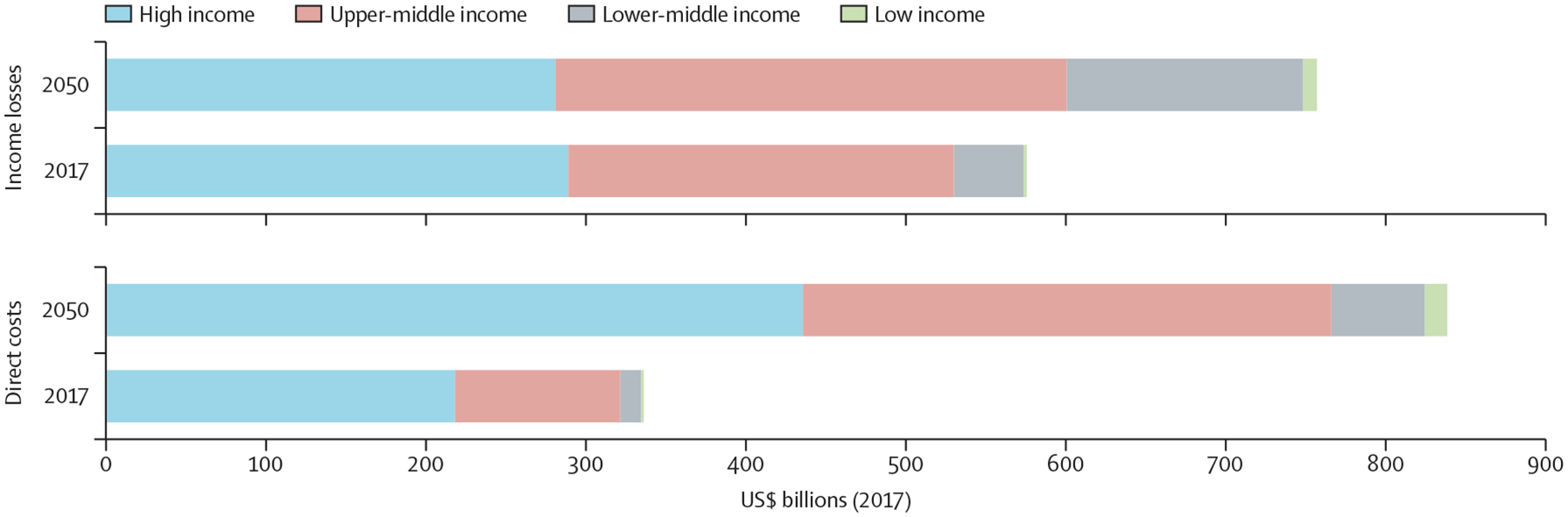
On the basis of our assessment, we have identified and prioritised several recommendations. For each of the four pillars (surveillance, prevention, acute care, and rehabilitation), we propose pragmatic solutions for the implementation of evidence-based interventions to reduce the global burden of stroke. The estimated direct (ie, treatment and rehabilitation) and indirect (considering productivity loss) costs of stroke globally are in excess of US$891 billion annually. The pragmatic solutions we put forwards for urgent implementation should help to mitigate these losses, reduce the global burden of stroke, and contribute to achievement of Sustainable Development Goal 3.4, the WHO Intersectoral Global Action Plan on epilepsy and other neurological disorders (2022–2031), and the WHO Global Action Plan for prevention and control of non-communicable diseases.
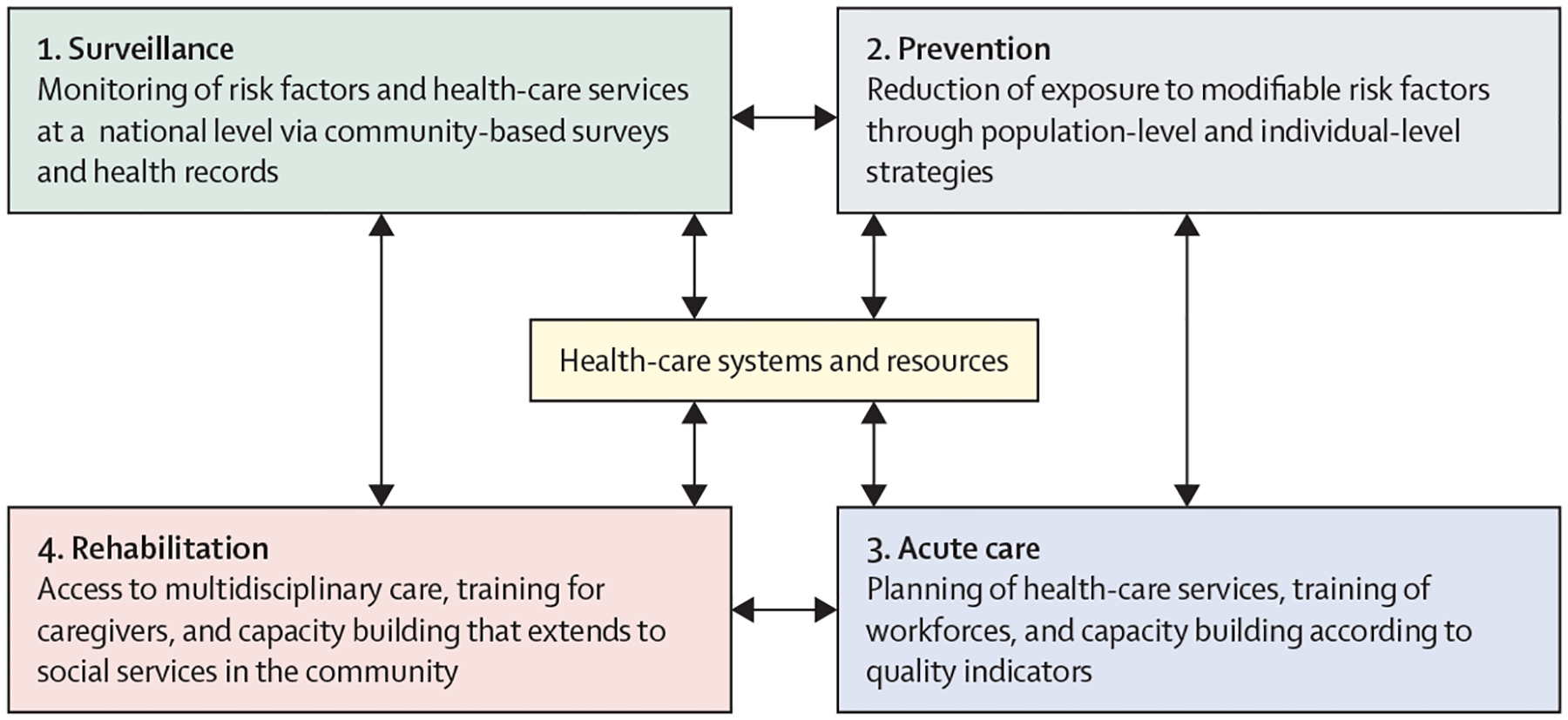
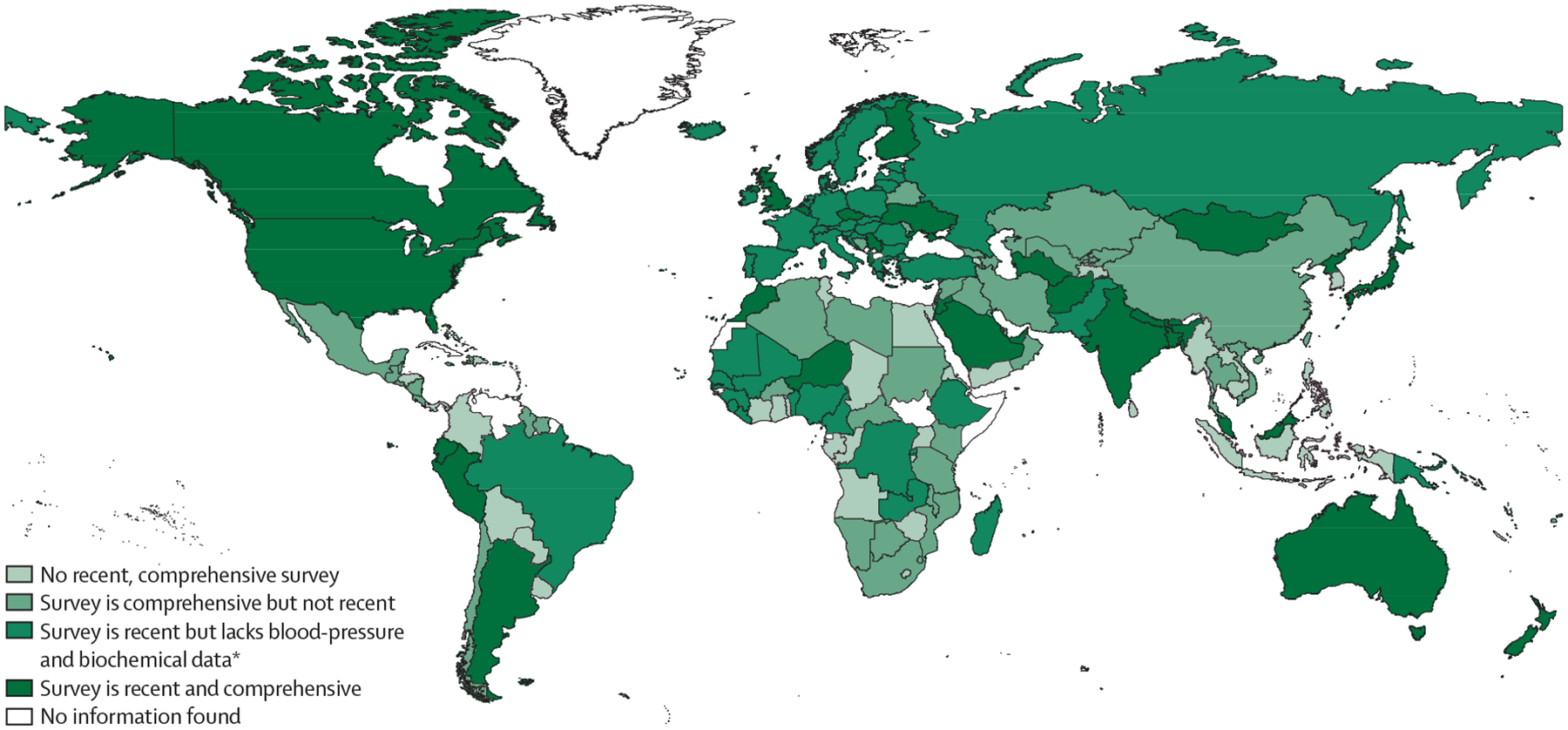
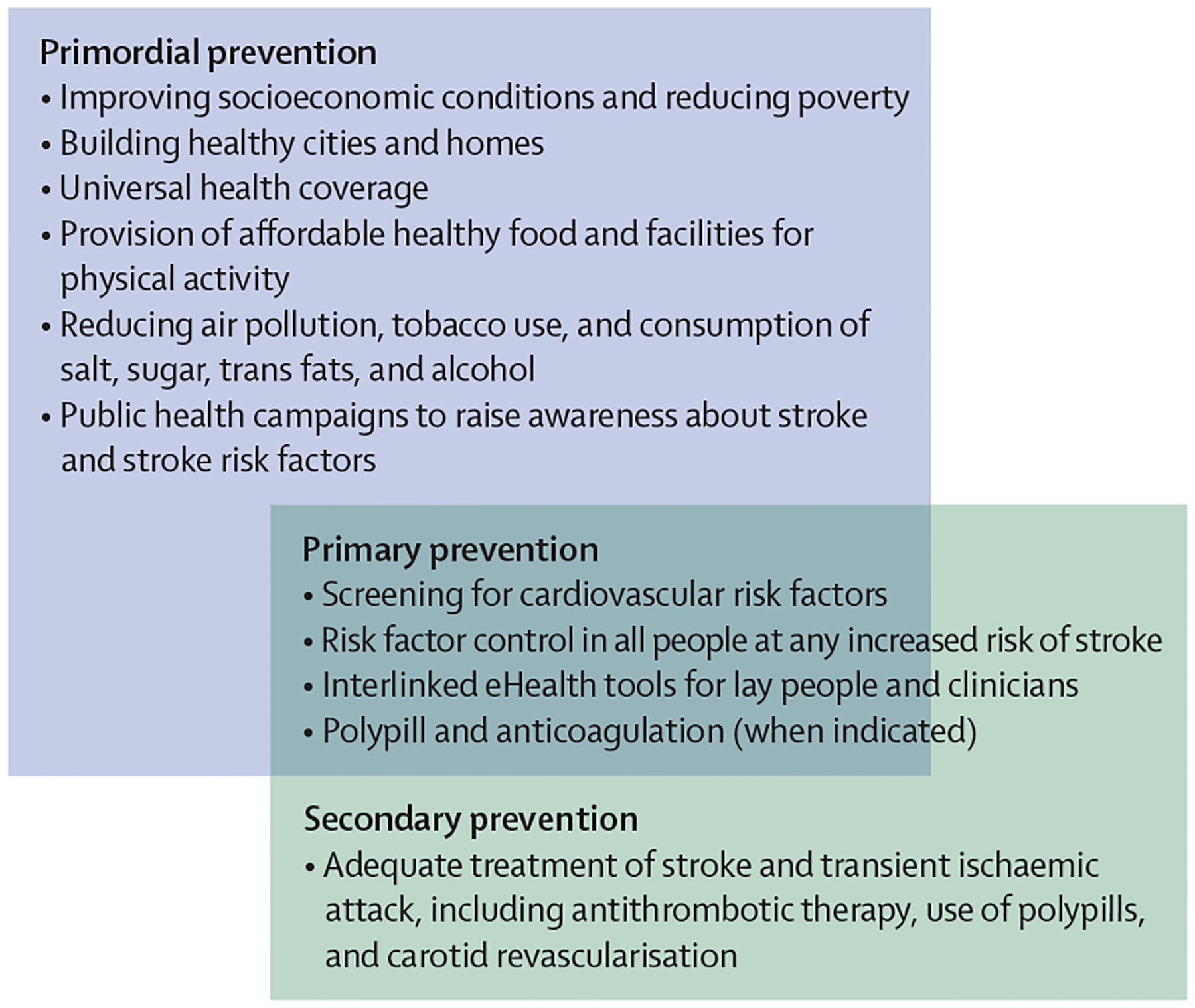
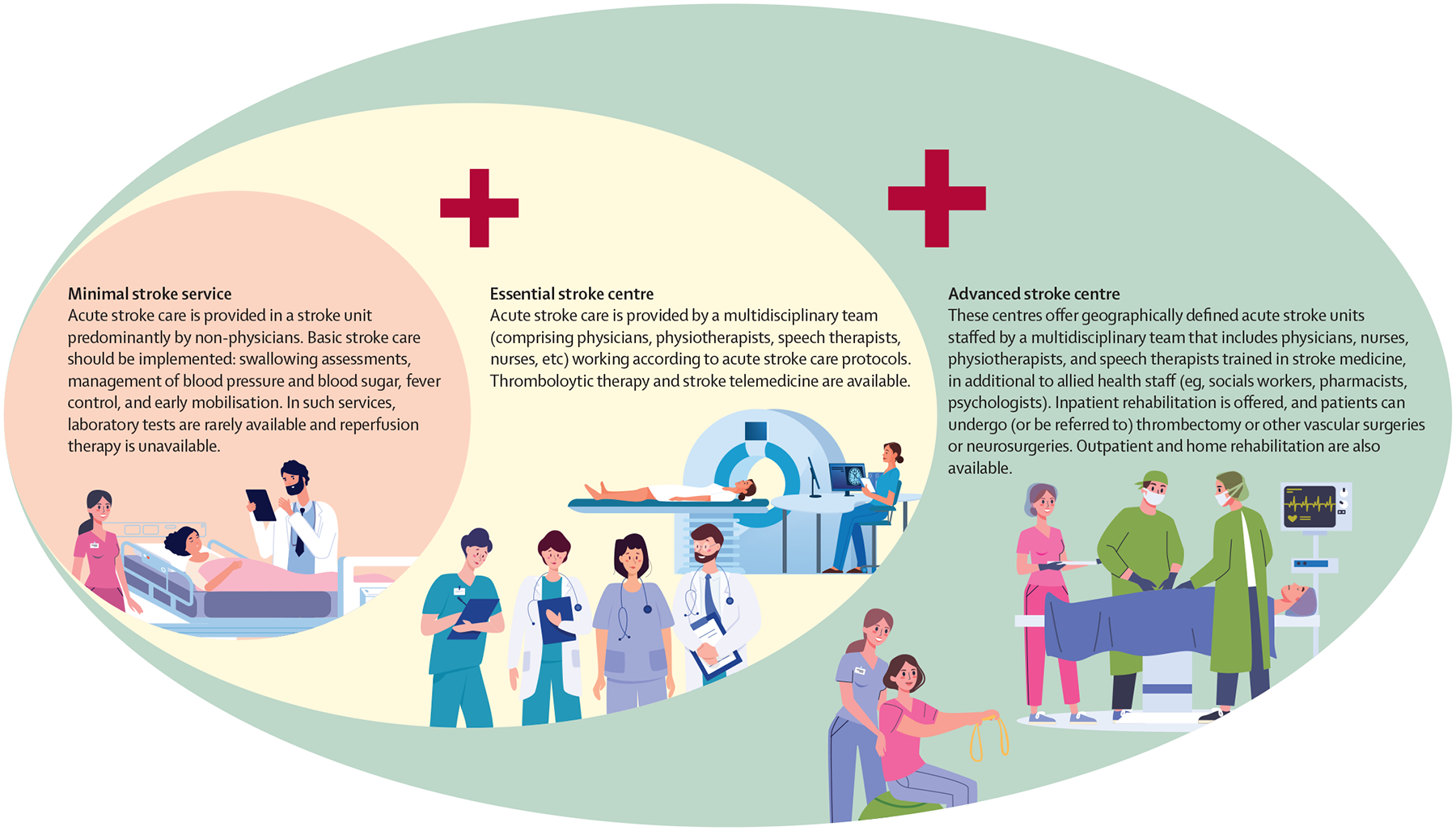
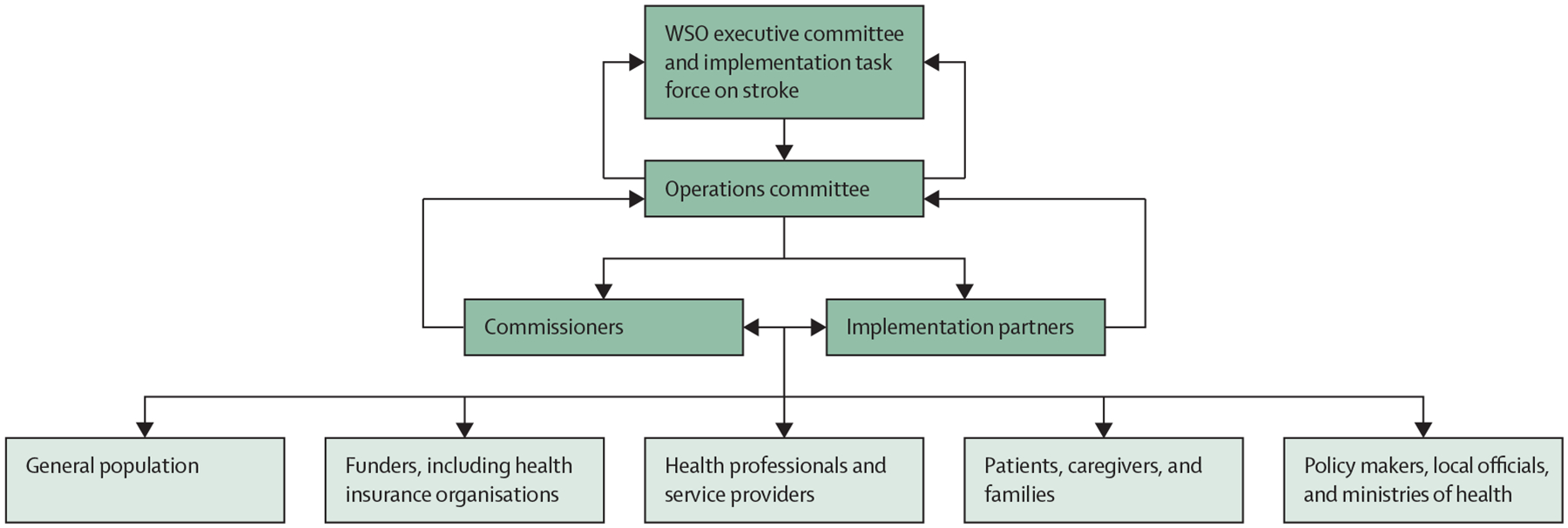
Reduction of the global burden of stroke, particularly in low-income and middle-income countries, by implementing primary and secondary stroke prevention strategies and evidence-based acute care and rehabilitation services is urgently required. Measures to facilitate this goal include: the establishment of a framework to monitor and assess the burden of stroke (and its risk factors) and stroke services at a national level; the implementation of integrated population-level and individual-level prevention strategies for people at any increased risk of cerebrovascular disease, with emphasis on early detection and control of hypertension; planning and delivery of acute stroke care services, including the establishment of stroke units with access to reperfusion therapies for ischaemic stroke and workforce training and capacity building (and monitoring of quality indicators for these services nationally, regionally, and globally); the promotion of interdisciplinary stroke care services, training for caregivers, and capacity building for community health workers and other health-care providers working in stroke rehabilitation; and the creation of a stroke advocacy and implementation ecosystem that includes all relevant communities, organisations, and stakeholders.
Conflict of interest statement
Declaration of interests VLF states that the free Stroke Riskometer app and PreventS-MD webapp are owned and copyrighted by AUT Ventures, which is owned by his employer, Auckland University of Technology (Auckland, New Zealand). VLF has no financial relationship with the apps, but AUT Ventures intends to commercialise PreventS-MD via its social enterprise business, for which VLF serves as chief scientific advisor. PreventS-MD was not involved in any aspect of the design, conduct, analysis, or content of this Commission. GAF has received grants from Novartis, consulting fees from CSL Behring, and honoraria from Astellas and Bayer; has served on data safety monitoring boards, data-monitoring committees, and steering committees for Pharmagenesis and Boehringer Ingelheim; and is a non-executive director of the UK National Institute for Health and Care Excellence and a trustee of Health Services Research UK. DCG has received travel support from the World Federation for Neurorehabilitation and Conventus Travel, and is a past president of the World Federation for Neurorehabilitation. WH has participated on data safety monitoring boards for IFS Institut für anwendungsorientierte Forschung und klinische Studien and Imperical College, London, and is a past president of the World Stroke Organization. GJH has received consultation fees from Janssen Research and Development, Bristol Myers Squibb, and Bayer, and has participated on data safety monitoring boards for Janssen Research and Development. PL has received honoraria from Pfizer, Boehringer Ingelheim, and RAPID-AI iSchemaView; has received travel support from Angels–Boehringer Ingelheim; has participated on data safety monitoring boards and steering committees for Pfizer and Janssen; and is the president of the Chilean Stroke Association and vice-president of the Iberoamerican Stroke Society. BN has received honoraria for serving on data safety monitoring boards work for Simbec-Orion. TP is a member of the Data Safety Monitoring Board for a publicly funded trial in Germany, with public grant money paid to his institution. AR has received honoraria from the University of Texas at Austin (Austin, TX, USA) and Medical College of Virginia (Richmond, VA, USA), and travel support from Fiji National University. PNS is a leader or member of advisory boards for Medtronic and the Angels Initiative (funded by Boehringer-Ingelheim). DY has served as consultant for the Athersys, Johnson & Johnson, Medtronic, Rapid Medical, Gravity Medical Technology, Guidepoint Global, Poseydon, Vascular Dynamics, Royal Caribbean Cruises, and Stryker; holds stocks or stock options in Athersys, Poseydon, and Rapid Medical; has received honoraria payments from Emory University (Atlanta, GA, USA); and is founder and global co-chair of the Society for Vascular and Interventional Neurology's Mission Thrombectomy. All other authors declare no competing interests.
Figures
Comment in
-
Policy priorities for preventing stroke-related mortality and disability worldwide.Lancet Neurol. 2023 Dec;22(12):1096-1098. doi: 10.1016/S1474-4422(23)00387-3. Epub 2023 Oct 9. Lancet Neurol. 2023. PMID: 37827181 No abstract available.
-
Balancing the scales of adversity: a socioecological approach to reducing the global burden of stroke and cardiovascular disease.Lancet Neurol. 2023 Dec;22(12):1094-1096. doi: 10.1016/S1474-4422(23)00386-1. Epub 2023 Oct 9. Lancet Neurol. 2023. PMID: 37827182 No abstract available.
-
Pragmatic solutions for the global burden of stroke.Lancet Neurol. 2024 Apr;23(4):333-334. doi: 10.1016/S1474-4422(24)00040-1. Lancet Neurol. 2024. PMID: 38508826 No abstract available.
-
Pragmatic solutions for the global burden of stroke.Lancet Neurol. 2024 Apr;23(4):334. doi: 10.1016/S1474-4422(24)00039-5. Lancet Neurol. 2024. PMID: 38508828 No abstract available.
References
-
- Medeiros GC, Roy D, Kontos N, Beach SR. Post-stroke depression: a 2020 updated review. Gen Hosp Psychiatry 2020; 66: 70–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
