

Survival Analysis of Immunotherapy Effects on Relapse Rate in Pediatric and Adult Autoimmune Encephalitis
- PMID: 37827848
- PMCID: PMC10727225
- DOI: 10.1212/WNL.0000000000207746
Survival Analysis of Immunotherapy Effects on Relapse Rate in Pediatric and Adult Autoimmune Encephalitis
Erratum in
-
Corrections to Received Date Information.Neurology. 2024 Jul 9;103(1):e209596. doi: 10.1212/WNL.0000000000209596. Epub 2024 Jun 3. Neurology. 2024. PMID: 38830175 Free PMC article. No abstract available.
Abstract
Background and objectives: Prior observational studies for autoimmune encephalitis (AE) have mostly focused on outcomes after acute immunotherapies with better outcomes associated with earlier immunotherapy use. However, the impact of long-term immunotherapy and its association with clinical relapse is not well known.
Methods: We conducted a retrospective study of consecutive patients meeting published clinical criteria for AE evaluated at UC San Diego and Rady Children's Hospital from January 2007 to November 2021. Survival analysis and Cox multivariable regression models were used to evaluate relapse risk using rituximab exposure as a time-dependent variable. Pooled and age-stratified analyses were performed.
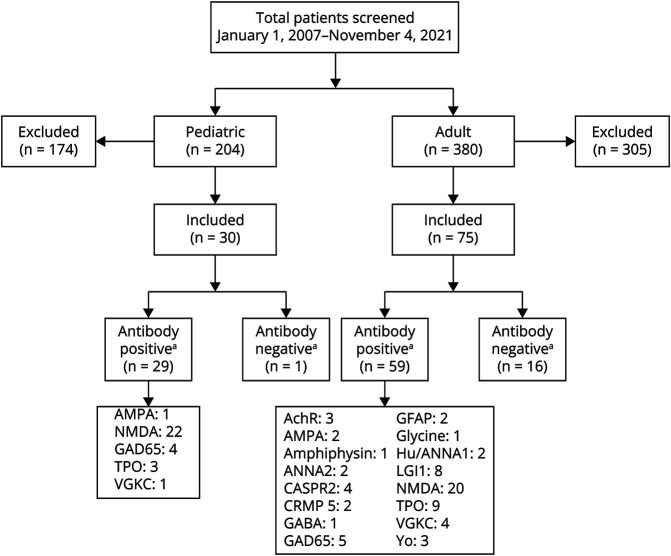
Results: A total of 204 pediatric and 380 adult participants were screened of which 30 pediatric and 75 adult participants were included. The most common antibody subtype in both cohorts was anti-NMDA receptor (76% in pediatric, 34% in adult). Relapses occurred in 31% of pediatric antibody-positive, 40% of adult antibody-positive, and 20% of adult antibody-negative cases. Times to first relapse (TTFR) were 10.6 ± 7.4 months (pediatric antibody-positive), 13.1 ± 24.5 months (adult antibody-positive), and 6.9 ± 3.8 months (adult antibody-negative). Rituximab was the most common second-line immunotherapy used. Combining pediatric and adult data, rituximab use was associated with a 71% lower hazard for time to first relapse (hazard ratio [HR] 0.29, 95% CI 0.09-0.85) and 51% lower hazard for recurring relapses (HR 0.49, 95% CI 0.9-1.26). The HR for TTFR with rituximab use in children was 0.30 (95% CI 0.05-1.69), 0.29 (95% CI 0.07-1.29) in adults, 0.32 in non-NMDA antibody-positive encephalitis (95% CI 0.07-1.39), and 0.42 (95% CI 0.07-2.67) for anti-NMDAR.
Discussion: Relapses are common in pediatric and adult patients with AE, although less frequently in anti-NMDARE. Using a rigorous survival model, we demonstrate a substantial benefit of rituximab use for reducing relapse rates in AE, especially for the adult population.
Classification of evidence: This study provides Class IV evidence that rituximab is associated with a lower hazard to relapse in patients with AE.
© 2023 American Academy of Neurology.
Conflict of interest statement
J.H. Yang, E. Liu, and L. Nguyen report no disclosures relevant to the manuscript; A. Dunn-Pirio reports no disclosures relevant to the manuscript; J.S. Graves has received grant or clinical trial funding from the NMSS, UCSD, Octave, Biogen, EMD-Serono, and ABM. She serves on a steering committee for a clinical trial with Novartis and served on advisory boards for TG therapeutics, Genentech, and Bayer unrelated to the current work. Go to
Figures

References
-
- Gable MS, Sheriff H, Dalmau J, Tilley DH, Glaser CA. The frequency of autoimmune N-methyl-D-aspartate receptor encephalitis surpasses that of individual viral etiologies in young individuals enrolled in the California Encephalitis Project. Clin Infect Dis. 2012;54(7):899-904. doi:10.1093/cid/cir1038 - DOI - PMC - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials