

Phase 2 Re-Entry Without Ito: Role of Sodium Channel Kinetics in Brugada Syndrome Arrhythmias
- PMID: 37831035
- PMCID: PMC11348283
- DOI: 10.1016/j.jacep.2023.08.027
Phase 2 Re-Entry Without Ito: Role of Sodium Channel Kinetics in Brugada Syndrome Arrhythmias
Abstract
Background: In Brugada syndrome (BrS), phase 2 re-excitation/re-entry (P2R) induced by the transient outward potassium current (Ito) is a proposed arrhythmia mechanism; yet, the most common genetic defects are loss-of-function sodium channel mutations.
Objectives: The authors used computer simulations to investigate how sodium channel dysfunction affects P2R-mediated arrhythmogenesis in the presence and absence of Ito.
Methods: Computer simulations were carried out in 1-dimensional cables and 2-dimensional tissue using guinea pig and human ventricular action potential models.
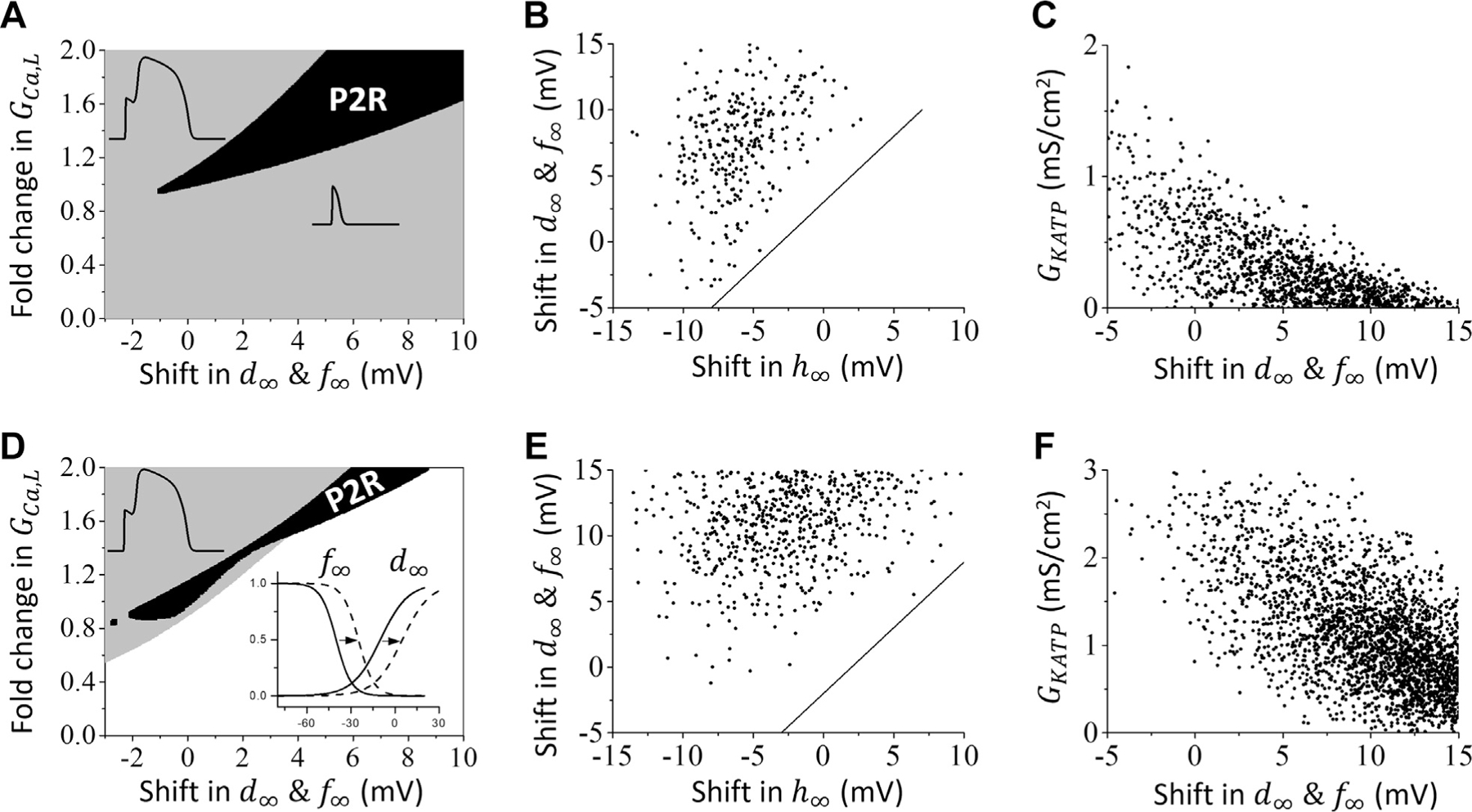
Results: In the presence of Ito sufficient to generate robust P2R, reducing sodium current (INa) peak amplitude alone only slightly potentiated P2R. When INa inactivation kinetics were also altered to simulate reported effects of BrS mutations and sodium channel blockers, however, P2R occurred even in the absence of Ito. These effects could be potentiated by delaying L-type calcium channel activation or increasing ATP-sensitive potassium current, consistent with experimental and clinical findings. INa-mediated P2R also accounted for sex-related, day and night-related, and fever-related differences in arrhythmia risk in BrS patients.
Conclusions: Altered INa kinetics synergize powerfully with reduced INa amplitude to promote P2R-induced arrhythmias in BrS in the absence of Ito, establishing a robust mechanistic link between altered INa kinetics and the P2R-mediated arrhythmia mechanism.
Keywords: Brugada syndrome; phase 2 re-entry; sodium channel blocker; sodium channel mutation.
Copyright © 2023 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by National Institutes of Health grants R01 HL134709, R01 HL133294, P01 HL164311, and R01 HL157116. Dr Zhang was supported by the National Natural Science Foundation of China Grants No. 12375033, No. 12235007 and No. 11975131, Zhejiang Provincial Natural Science Foundation of China under Grant No. LY23A050002; and K. C. Wong Magna Fund at Ningbo University. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures







Comment in
-
Phase-2 Re-Entry in Brugada Syndrome: More to Understand Than "Just" Ito.JACC Clin Electrophysiol. 2023 Dec;9(12):2475-2476. doi: 10.1016/j.jacep.2023.10.030. JACC Clin Electrophysiol. 2023. PMID: 38151299 No abstract available.
References
-
- Antzelevitch C, Brugada P, Brugada J, et al. Brugada syndrome: a decade of progress. Circ Res 2002;91:1114–1118. - PubMed
-
- Sieira J, Dendramis G, Brugada P. Pathogenesis and management of Brugada syndrome. Nat Rev Cardiol 2016;13:744–756. - PubMed
-
- Brugada J, Campuzano O, Arbelo E, Sarquella-Brugada G, Brugada R. Present status of Brugada syndrome. J Am Coll Cardiol 2018;72:1046–1059. - PubMed
-
- Nademanee K, Wilde AAM. Repolarization versus depolarization defects in Brugada syndrome. J Am Conll Cardiol EP 2017;3:364–366. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
