

Posttreatment liver function, but not baseline liver function stratifies patient survival after direct-acting antiviral treatment in decompensated cirrhosis with hepatitis C virus
- PMID: 37831182
- PMCID: PMC10657790
- DOI: 10.1007/s00535-023-02039-x
Posttreatment liver function, but not baseline liver function stratifies patient survival after direct-acting antiviral treatment in decompensated cirrhosis with hepatitis C virus
Abstract
Background: The prognosis of cirrhosis is clearly stratified by liver function. Although direct-acting antiviral (DAA) has recently been used to eliminate hepatitis C virus (HCV), it is not clear whether liver function stratifies the prognosis of decompensated cirrhotic patients treated with DAA.
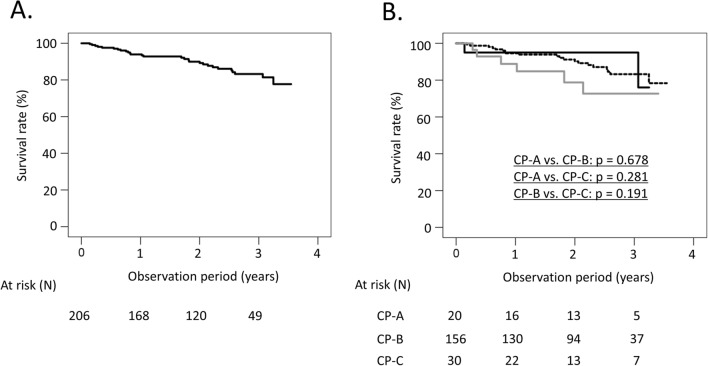
Methods: A total of 206 HCV-associated decompensated cirrhotic patients who started DAA from February 2019 to December 2021 at 31 Japanese hospitals were prospectively registered.
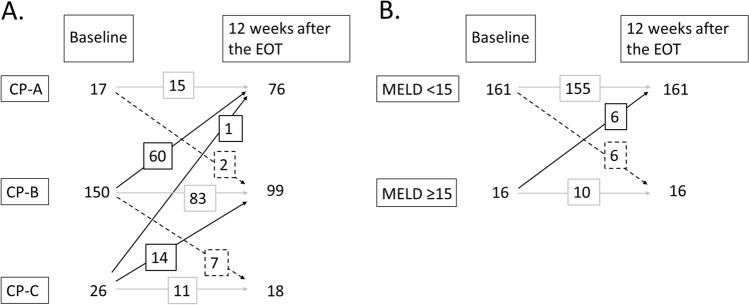
Results: The median age was 68, and the proportions of patients with Child-Pugh class A (CP-A), CP-B and CP-C were 10% (20/206), 76% (156/206) and 15% (30/206), respectively. Twenty-six patients died, and two patients underwent liver transplantation (LT); the 2- and 3-year LT-free survival rates were 90.0% and 83.2%, respectively. We examined factors associated with LT-free survival using 2 models including either CP class (Model 1) or MELD score (Model 2). In multivariate Cox proportional hazard analysis, CP class at 12 weeks after the end of treatment (EOT) in Model 1 and MELD score at 12 weeks after the EOT in Model 2 were significant factors, while baseline CP class or MELD score was not. Two-year LT-free survival rates were 100%, 91.6% and 60.4% for patients with CP-A, CP-B and CP-C at 12 weeks after the EOT and 95.2% and 69.6% for patients with MELD < 15 and MELD ≥ 15 at 12 weeks after the EOT, respectively.
Conclusions: The prognosis of decompensated cirrhotic patients receiving DAA was stratified by liver function at 12 weeks after the EOT, not by baseline liver function.
Keywords: Child–Pugh score; DAA; Prognosis; Sofosbuvir; Velpatasvir.
© 2023. The Author(s).
Conflict of interest statement
Satoshi Mochida received lecture fees from Gilead Sciences, Inc., AbbVie GK., ASKA Pharmaceutical Co., Ltd., Toray Industries Inc., Otuska Pharmaceutical Co., Ltd. and Eisai Co., Ltd. Masayuki Kurosaki received lecture fees from Gilead, AbbVie, Eisai, Chugai, AstraZeneca, Lilly and Takeda. Norifumi Kawada received research grants from AstraZeneca plc., Bristol Myers Squibb., Glaxosmithkline plc., MSD co., ltd., Gilead Sciences. Inc. and NovoNordisk pharma Ltd., scholarship grants from AbbVie GK, Eisai Co., Ltd. and Otsuka Pharmaceutical Co. and received lecture fees from AbbVie GK, Gilead Sciences, Inc. and MSD Co., Ltd. Goki Suda received research grants from Gilead Sciences Inc. Hitoshi Yoshiji received lecture fees from Gilead Sci. Naoya Kato received research grants from AbbVie G.K., scholarship grants from Gilead Sciences Inc., and lecture fees from Gilead Sciences, Inc. and AbbVie G.K. Taro Takami received lecture fees from Gilead Sciences, Inc. Yasuhiro Asahina belongs to a donation-funded department funded by Fujirebio Inc. and Abbott Japan LLC. Yoshito Itoh received research grants from Merck Sharp and Dohme., scholarship grants from AbbVie Inc. and Takeda Pharm. Co.Ltd. and lecture fees from AbbVie Inc and Gilead Sciences Inc. Shuji Terai received lecture fees from Otsuka, AbbVie, Asuka, Daiichisankyo, Chiomu Takedansen and Gilead. Yoshiyuki Ueno received lecture fees from AbbVie Inc. Norio Akuta received lecture fees from AbbVie Inc. Tetsuo Takehara received research grants and lecture fees from AbbVie GK. and Gilead Sciences, Inc. All other authors declare that they have no conflicts of interest to disclose.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
