

Obesity and Risk of Recurrence in Patients With Breast Cancer Treated With Aromatase Inhibitors
- PMID: 37831449
- PMCID: PMC10576219
- DOI: 10.1001/jamanetworkopen.2023.37780
Obesity and Risk of Recurrence in Patients With Breast Cancer Treated With Aromatase Inhibitors
Abstract
Importance: Clinical studies confirm that obesity is a risk factor for recurrence in postmenopausal women with hormone receptor-positive (HR+) breast cancer. Evidence suggests that women with obesity do not obtain similar protection from aromatase inhibitors as women with healthy weight.
Objective: To examine the associations of body mass index (BMI) with recurrence.
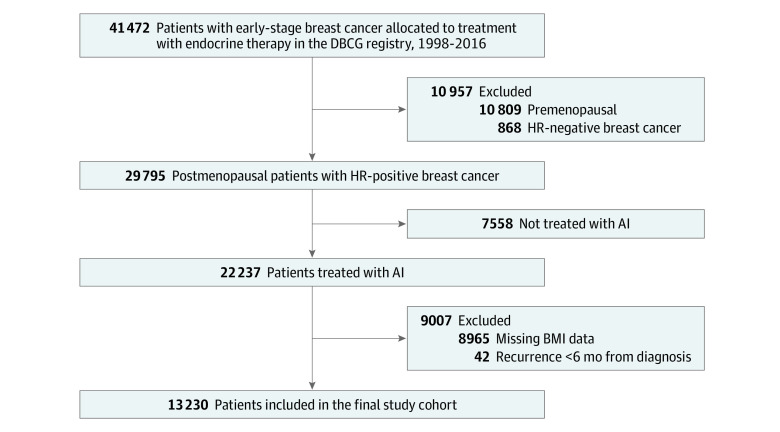
Design, setting, and participants: The cohort study was conducted using data from the Danish Breast Cancer Group and enrolled postmenopausal women diagnosed with stage I to III HR+ breast cancer from 1998 through 2016. Data analysis was conducted from November 2022 to April 2023.
Exposures: BMI was classified as (1) healthy weight (18.5-24.9), (2) overweight (25.0-29.9), (3) obesity (30.0-34.9), and (4) severe obesity (≥35.0) using the World Health Organization guidelines. Healthy weight was considered the reference group in statistical analyses.
Main outcomes and measures: Follow-up began 6 months after breast cancer surgery and continued until the first event of recurrence, contralateral breast cancer, new primary malignant neoplasm, death, emigration, end of clinical follow-up at 10 years, or September 25, 2018. Cox regression was used to estimate crude and adjusted hazard ratios with 95% CIs, adjusting for patient, tumor, and treatment characteristics.
Results: A total of 13 230 patients (median [IQR] age at diagnosis, 64.4 [58.6-70.2] years) with information on BMI were enrolled. There were 1587 recurrences with a median (IQR) potential estimated follow-up of 6.2 (3.6-8.5) years. Multivariable analyses revealed increased recurrence hazards associated with obesity (adjusted hazard ratio, 1.18 [95% CI, 1.01-1.37]) and severe obesity (adjusted hazard ratio, 1.32 [95% CI, 1.08-1.62]) vs patients with healthy weight. Patients with overweight had a greater risk, but the results were not statistically significant (adjusted hazard ratio, 1.10 [95% CI, 0.97-1.24]).
Conclusions and relevance: In this study, obesity was associated with an increased risk of breast cancer recurrence among postmenopausal patients with HR+ early-stage breast cancer treated with aromatase inhibitors. Physicians should be aware of the significance of obesity on breast cancer outcomes to secure optimal treatment benefit in all patients.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
