

Retrospective cohort analysis of outpatient antibiotic prescribing for community-acquired pneumonia in Canadian older adults
- PMID: 37831711
- PMCID: PMC10575505
- DOI: 10.1371/journal.pone.0292899
Retrospective cohort analysis of outpatient antibiotic prescribing for community-acquired pneumonia in Canadian older adults
Abstract
Background: This retrospective cohort study is the first in North America to examine population-level appropriate antibiotic use for community-acquired pneumonia (CAP) in older adults, by agent, dose and duration. With the highest rates of CAP reported in the elderly populations, appropriate antibiotic use is essential to improve clinical outcomes. Given the ongoing crisis of antimicrobial resistance, understanding inappropriate antibiotic prescribing is integral to direct community stewardship efforts.
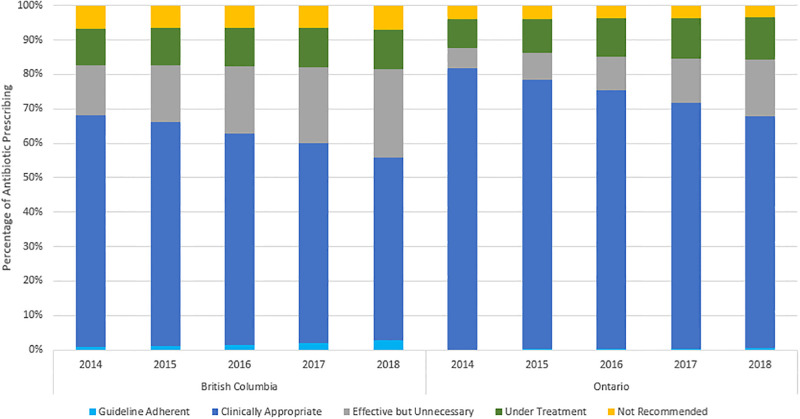
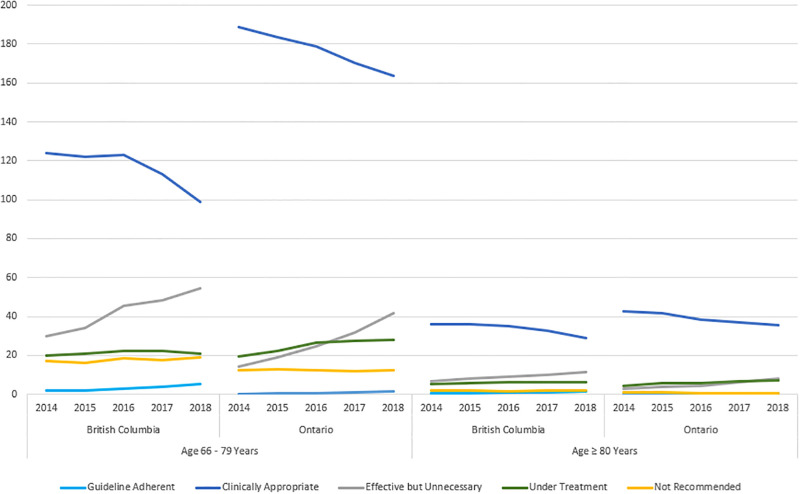
Methods: All outpatient primary care visits for CAP (aged ≥65 years) were identified using physician billing codes between January 1 2014 to December 31 2018 in British Columbia (BC) and Ontario (ON). Categories of prescribing were derived from existing literature, and constructed for clinical relevance using Canadian and international guidelines available during the study period. Categories were mutually exclusive and included: guideline adherent (first-line agent, adherent dose/duration), clinically appropriate (non-first line agent, presence of comorbidities), effective but unnecessary (first-line agent, excess dose/duration), undertreatment (first-line agent, subtherapeutic dose/duration), and not recommended (non-first line agent, absence of comorbidities). Proportions of prescribing were examined by category. Temporal trends in prescribing were examined using Poisson regression.
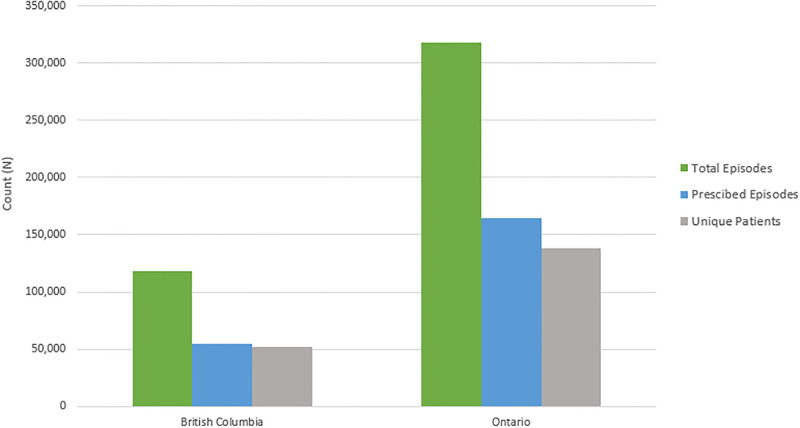
Results: A total of 436,441 episodes of CAP were identified, with 46% prescribed an antibiotic in BC, and 52% in Ontario. Guideline adherent prescribing was minimal for both provinces (BC: 2%; ON: 1%) however the largest magnitude of increase was reported in this category by the final study year (BC-Rate Ratio [RR]: 3.4, 95% Confidence Interval [CI]: 2.7-4.3; ON-RR: 4.62, 95% CI: 3.4-6.5). Clinically appropriate prescribing accounted for the most antibiotics issued, across all study years (BC: 61%; ON: 74%) (BC-RR: 0.8, 95% CI: 0.8-0.8; ON-RR: 0.9, 95% CI: 0.8-0.9). Excess duration of therapy was the hallmark characteristic for effective but unnecessary prescribing (BC: 92%; ON: 99%). The most common duration prescribed was 7 days, followed by 10. Not recommended prescribing was minimal in both provinces (BC: 4%; ON: 7%) and remained stable by the final study year (BC-RR: 1.1, 95% CI: 0.9-1.2; ON-RR: 0.9, 95% CI: 0.9-1.1).
Conclusion: Three quarters of antibiotic prescribing for CAP was appropriate in Ontario, but only two thirds in BC. Shortening durations-in line with evidence for 3 to 5-day treatment presents a focused target for stewardship efforts.
Copyright: © 2023 Saatchi et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared no competing interests exist.
Figures
References
-
- S. Jain et al., “Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults,” 10.1056/NEJMoa1500245. Accessed: Apr. 29, 2021. [Online]. https://www.nejm.org/doi/10.1056/NEJMoa1500245 - DOI - DOI
-
- Musher D. M., Abers M. S., and Bartlett J. G., “Evolving Understanding of the Causes of Pneumonia in Adults, With Special Attention to the Role of Pneumococcus,” Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am., vol. 65, no. 10, pp. 1736–1744, Nov. 2017, doi: 10.1093/cid/cix549 - DOI - PMC - PubMed
-
- Musher D. M., Roig I. L., Cazares G., Stager C. E., Logan N., and Safar H., “Can an etiologic agent be identified in adults who are hospitalized for community-acquired pneumonia: Results of a one-year study,” J. Infect., vol. 67, no. 1, pp. 11–18, Jul. 2013, doi: 10.1016/j.jinf.2013.03.003 - DOI - PMC - PubMed
-
- Johansson N., Kalin M., Tiveljung-Lindell A., Giske C. G., and Hedlund J., “Etiology of Community-Acquired Pneumonia: Increased Microbiological Yield with New Diagnostic Methods,” Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am., vol. 50, no. 2, pp. 202–209, Jan. 2010, doi: 10.1086/648678 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
