

Predictive Value of Fibrin Fibrinogen Degradation Products-to-Potassium Ratio for Poor Functional Outcome in Patients with Aneurysmal Subarachnoid Hemorrhage: A Retrospective Case-Control Study
- PMID: 37833519
- PMCID: PMC11147889
- DOI: 10.1007/s12028-023-01865-4
Predictive Value of Fibrin Fibrinogen Degradation Products-to-Potassium Ratio for Poor Functional Outcome in Patients with Aneurysmal Subarachnoid Hemorrhage: A Retrospective Case-Control Study
Abstract
Background: The relationship of fibrin(ogen) degradation products (FDPs) and potassium with the functional outcomes of patients with aneurysmal subarachnoid hemorrhage (aSAH) is still uncertain. This study aims to evaluate the predictive value of a novel combination biomarker, the FDP-to-potassium ratio (FPR), for poor functional outcomes in patients with aSAH.
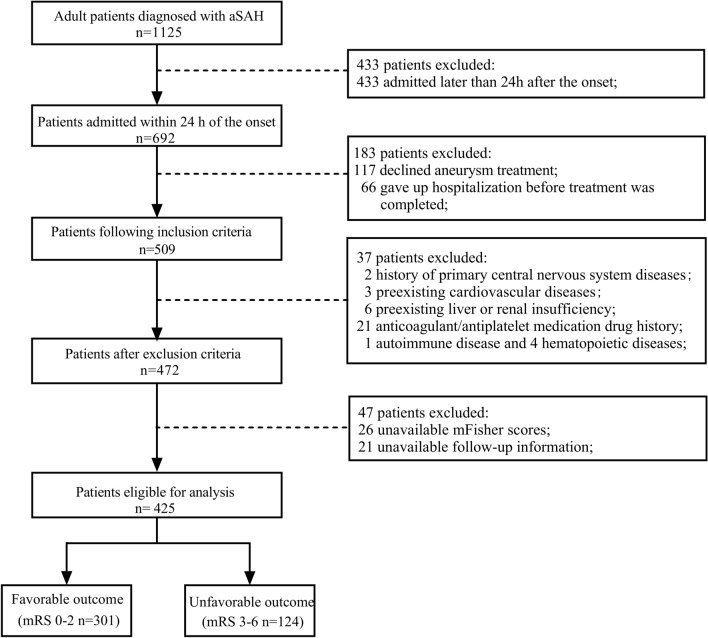
Methods: A total of 425 consecutive patients with aSAH at a single center were retrospectively enrolled in our study. An unfavorable outcome was defined as a modified Rankin Scale (mRS) score of 3-6 at 3 months after discharge. Univariate analysis and multivariable logistic regression were performed for baseline information and laboratory parameters recorded at admission. In addition, the receiver operating characteristic curve was plotted, and propensity score matching was performed based on the FPR.
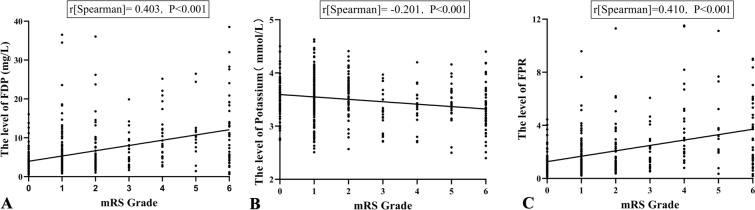
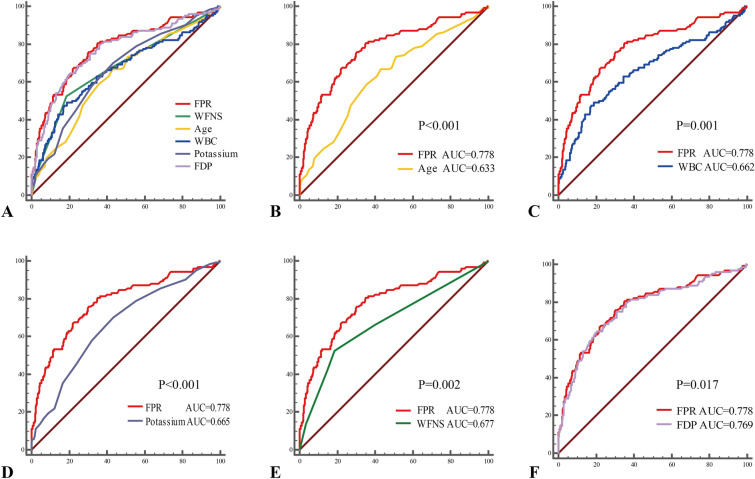
Results: On the basis of mRS grade, 301 patients were classified as having favorable outcomes, and 124 patients were assessed as having unfavorable outcomes. FPR levels were significantly correlated with mRS grade (r[Spearman] = 0.410; P < 0.001). Multivariate logistic regression analysis showed that age (odds ratio [OR] 1.043, 95% confidence interval [CI] 1.016-1.071; P = 0.002), white blood cell count (OR 1.150, 95% CI 1.044-1.267; P = 0.005), potassium (OR 0.526, 95% CI 0.291-0.949; P = 0.033), World Federation of Neurosurgical Societies grade (OR 1.276, 95% CI 1.055-1.544; P = 0.012), and FPR (OR 1.219, 95% CI 1.102-1.349; P < 0.001) at admission were independently associated with poor functional outcomes. The DeLong test showed that the area under the receiver operating characteristic curve of FPR was higher than that of age, white blood cell count, potassium, World Federation of Neurosurgical Societies grade, or FDP alone, indicating that FPR had better predictive potential than these other variables. After 1:1 propensity score matching (FPR ≥ 1.45 vs. FPR < 1.45), the rate of poor prognosis was still significantly increased in the high-FPR group (48/121 [39.7%] vs. 16/121 [13.2%], P < 0.001).
Conclusions: Fibrin(ogen) degradation product-to-potassium ratio is an independent predictor of poor outcomes for patients with aSAH and may be a promising tool for clinicians to evaluate patients' functional prognosis.
Keywords: Aneurysmal subarachnoid hemorrhage; Fibrin fibrinogen degradation products; Hypokalemia; Outcome; Potassium; Predict.
© 2023. The Author(s).
Conflict of interest statement
All authors declare that we have no conflicts of interest.
Figures



References
MeSH terms
Substances
Grants and funding
- 202210634045/National College Students Innovation and Entrepreneurship Training Program
- 202210634026/National College Students Innovation and Entrepreneurship Training Program
- 20SXKT0317/Cooperation Project of Nanchong City and North Sichuan Medical College
- CBY-20-QA-Z02/Research development program of North Sichuan Medical College
LinkOut - more resources
Full Text Sources
Medical
