

Procalcitonin-guided antibiotic therapy may shorten length of treatment and may improve survival-a systematic review and meta-analysis
- PMID: 37833778
- PMCID: PMC10576288
- DOI: 10.1186/s13054-023-04677-2
Procalcitonin-guided antibiotic therapy may shorten length of treatment and may improve survival-a systematic review and meta-analysis
Abstract
Background: Appropriate antibiotic (AB) therapy remains a challenge in the intensive care unit (ICU). Procalcitonin (PCT)-guided AB stewardship could help optimize AB treatment and decrease AB-related adverse effects, but firm evidence is still lacking. Our aim was to compare the effects of PCT-guided AB therapy with standard of care (SOC) in critically ill patients.
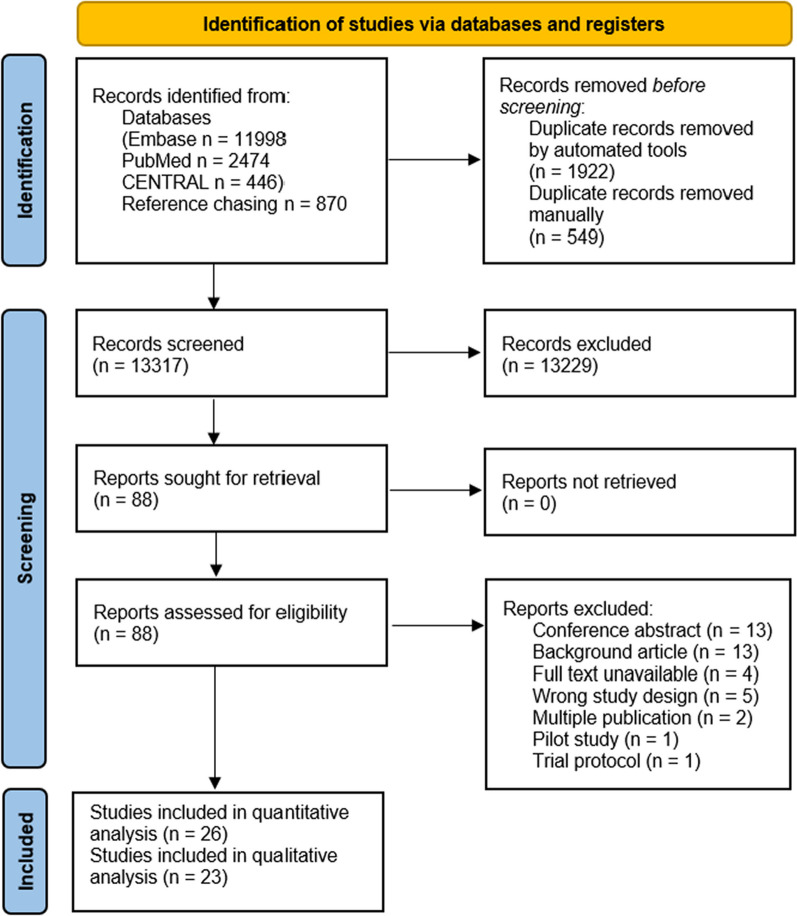
Methods: We searched databases CENTRAL, Embase and Medline. We included randomized controlled trials (RCTs) comparing PCT-guided AB therapy (PCT group) with SOC reporting on length of AB therapy, mortality, recurrent and secondary infection, ICU length of stay (LOS), hospital LOS or healthcare costs. Due to recent changes in sepsis definitions, subgroup analyses were performed in studies applying the Sepsis-3 definition. In the statistical analysis, a random-effects model was used to pool effect sizes.
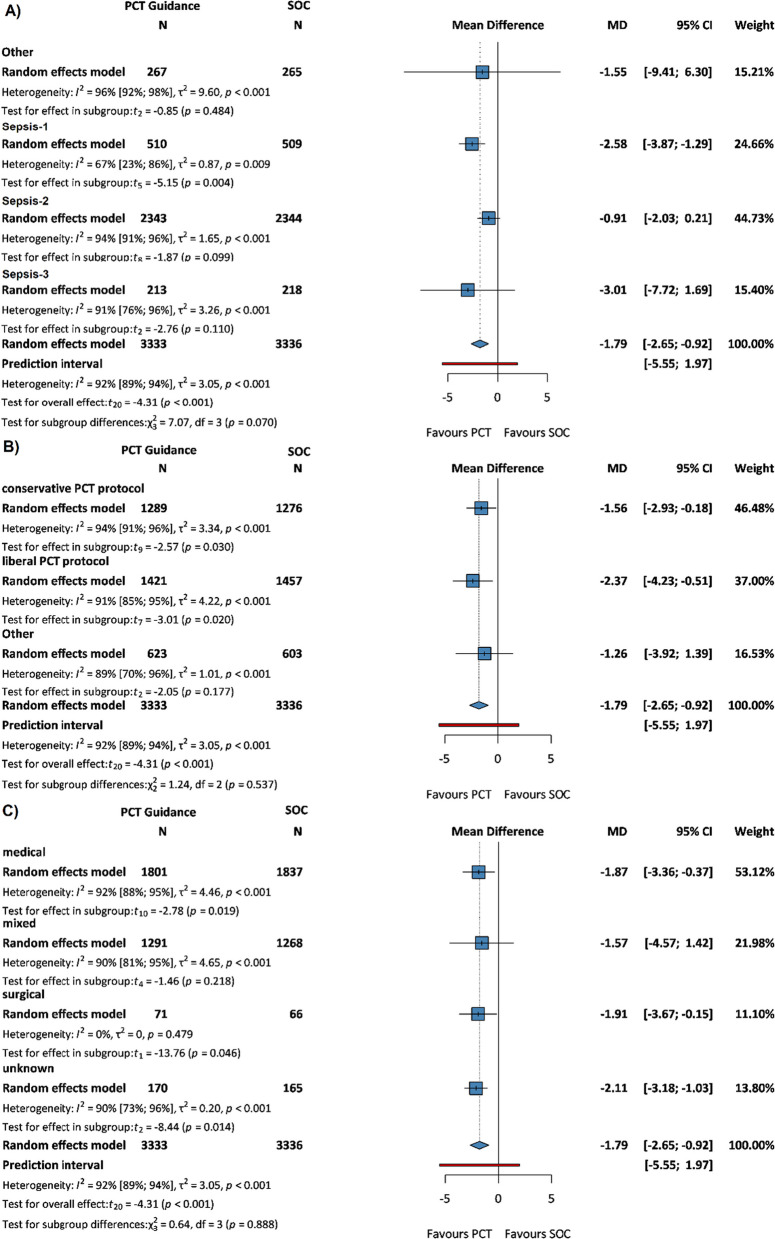
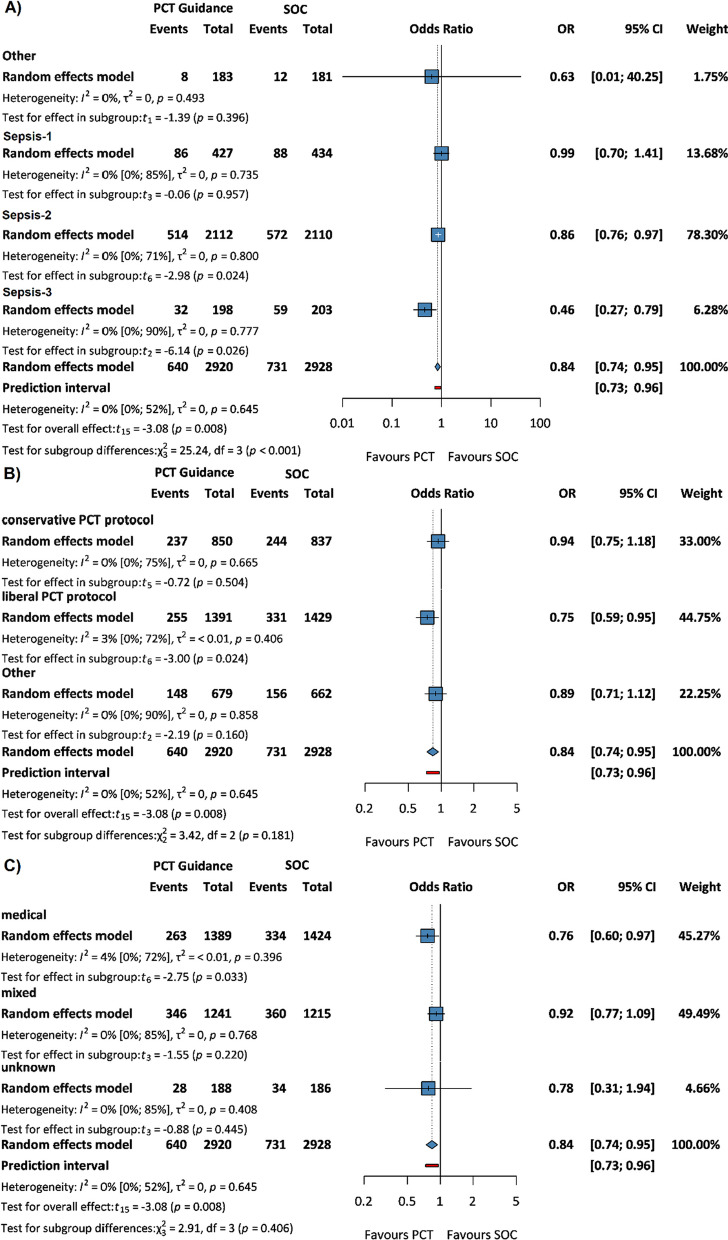
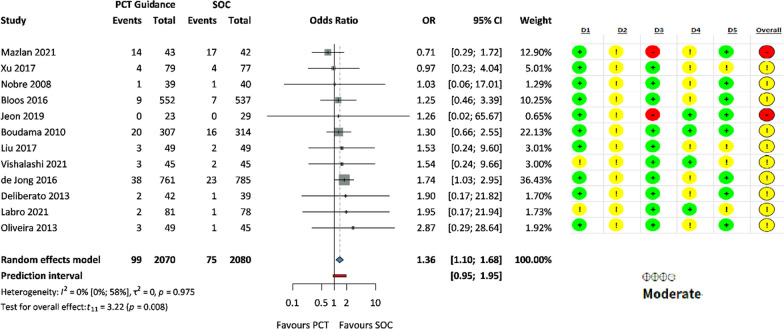
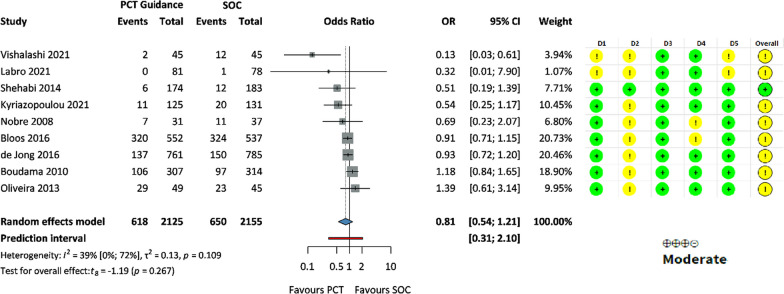
Results: We included 26 RCTs (n = 9048 patients) in the quantitative analysis. In comparison with SOC, length of AB therapy was significantly shorter in the PCT group (MD - 1.79 days, 95% CI: -2.65, - 0.92) and was associated with a significantly lower 28-day mortality (OR 0.84, 95% CI: 0.74, 0.95). In Sepsis-3 patients, mortality benefit was more pronounced (OR 0.46 95% CI: 0.27, 0.79). Odds of recurrent infection were significantly higher in the PCT group (OR 1.36, 95% CI: 1.10, 1.68), but there was no significant difference in the odds of secondary infection (OR 0.81, 95% CI: 0.54, 1.21), ICU and hospital length of stay (MD - 0.67 days 95% CI: - 1.76, 0.41 and MD - 1.23 days, 95% CI: - 3.13, 0.67, respectively).
Conclusions: PCT-guided AB therapy may be associated with reduced AB use, lower 28-day mortality but higher infection recurrence, with similar ICU and hospital length of stay. Our results render the need for better designed studies investigating the role of PCT-guided AB stewardship in critically ill patients.
Keywords: Antibiotic therapy; Intensive care; Procalcitonin; Sepsis.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- De Waele JJ, Boelens J, Leroux-Roels I. Multidrug-resistant bacteria in ICU: fact or myth. Curr Opin Anaesthesiol. 2020;33:156–161. - PubMed
-
- Vincent J-L, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302:2323–2329. - PubMed
-
- Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49:e1063–e1143. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
