

Transcranial Magnetic Stimulation for the Treatment of Chemo Brain
- PMID: 37836847
- PMCID: PMC10575384
- DOI: 10.3390/s23198017
Transcranial Magnetic Stimulation for the Treatment of Chemo Brain
Abstract
This pilot feasibility study aimed to evaluate the effects of transcranial magnetic stimulation (TMS) on chemotherapy-related cognitive impairment (CRCI), and we report here on the first patient.
Background: Deleterious cognitive changes due to chemotherapy or CRCI are commonly referred to as "chemo brain". With the increasing survival of cancer patients, this poorly understood and inadequately treated condition will likewise have an increasing toll on individuals and society. Since there is no approved treatment for chemo brain, we have initiated a therapeutic trial using transcranial magnetic stimulation (TMS), a non-invasive brain stimulation technique approved in many countries for the treatment of neurologic and psychiatric conditions like migraine and depression.
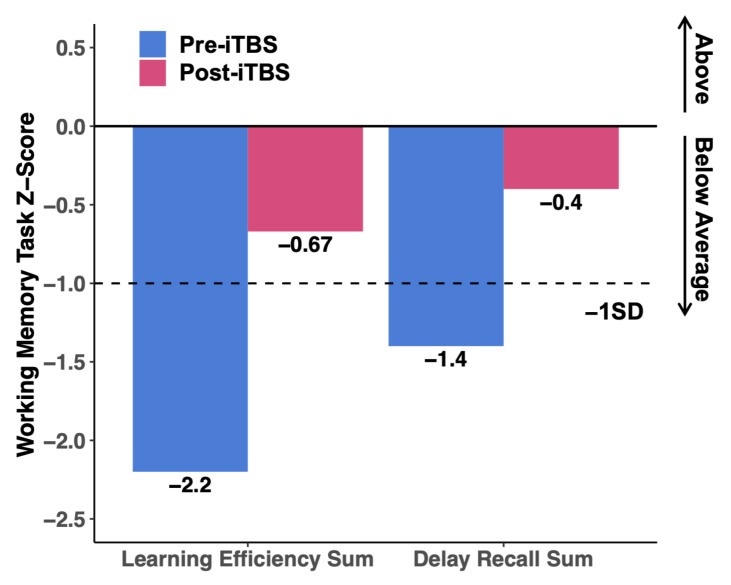
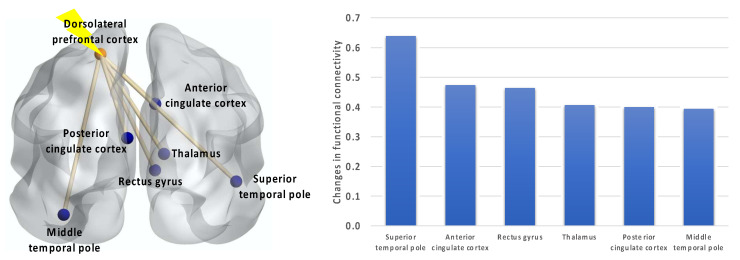
Case presentation: A 58-year-old woman, diagnosed 7 years prior with left breast cancer, underwent partial mastectomy with sentinel lymph node biopsy. She then received four cycles of adjuvant chemotherapy followed by radiation therapy. Afterwards, she was on tamoxifen for 4 years and then switched to aromatase inhibitors. The patient's CRCI started during chemotherapy and severely impaired her quality of life for an additional two years. In the third year after chemotherapy, the CRCI partially cleared to stabilize to the level at the time of presentation for this trial. The patient continues to have memory difficulties and decreased concentration, which makes multi-tasking very difficult to impossible. She is reliant on memory aids at work and at home. The participant underwent 10 consecutive sessions of TMS during weekdays for 2 weeks. Stimulation was directed to the left dorsolateral prefrontal cortex. After TMS, the participant significantly improved in memory function on neuropsychological testing. While she reported no subjective differences in concentration or memory, she did report an improvement in her sleep. Functional magnetic resonance imaging of the brain before and after TMS showed increased resting-state functional connectivity between the stimulation site and several brain regions. Remarkably, after 6 years of chemo brain and remaining in the same position at work due to her inability to concentrate and multi-task, she applied for and received a promotion 5-6 months after her TMS treatments.
Conclusions: This first patient in the phase 1 clinical trial testing of TMS for the treatment of "chemo brain" provided important lessons for feasibility and insights into mechanisms of potential benefit.
Keywords: chemo brain; chemotherapy-related cognitive impairment; transcranial magnetic stimulation.
Conflict of interest statement
P.H. Kuo is a consultant and/or speaker for Blue Earth Diagnostics, Chimerix, Eli Lilly, Fusion Pharma, General Electric Healthcare, Invicro, Novartis, Radionetics, and Telix Pharmaceuticals. He is a recipient of research grants from Blue Earth Diagnostics and General Electric Healthcare. The other authors declare that they have no financial interests.
Figures
References
-
- Argyriou A.A., Assimakopoulos K., Iconomou G., Giannakopoulou F., Kalofonos H.P. Either called “chemobrain” or “chemofog”, the long-term chemotherapy-induced cognitive decline in cancer survivors is real. J. Pain Symptom. Manag. 2011;41:126–139. doi: 10.1016/j.jpainsymman.2010.04.021. - DOI - PubMed
-
- Saykin A., Ahles T., McDonald B. Mechanisms of Chemotherapy-Induced Cognitive Disorders: Neuropsychological, Pathophysiological, and Neuroimaging Perspectives. Semin. Clin. Neuropsychiatry. 2003;8:201–216. - PubMed
-
- Cimprich B., Reuter-Lorenz P., Nelson J., Clark P.M., Therrien B., Normolle D., Berman M.G., Hayes D.F., Noll D.C., Peltier S., et al. Prechemotherapy alterations in brain function in women with breast cancer. J. Clin. Exp. Neuropsychol. 2010;32:324–331. doi: 10.1080/13803390903032537. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
