

Cefepime vs Piperacillin-Tazobactam in Adults Hospitalized With Acute Infection: The ACORN Randomized Clinical Trial
- PMID: 37837651
- PMCID: PMC10576861
- DOI: 10.1001/jama.2023.20583
Cefepime vs Piperacillin-Tazobactam in Adults Hospitalized With Acute Infection: The ACORN Randomized Clinical Trial
Abstract
Importance: Cefepime and piperacillin-tazobactam are commonly administered to hospitalized adults for empirical treatment of infection. Although piperacillin-tazobactam has been hypothesized to cause acute kidney injury and cefepime has been hypothesized to cause neurological dysfunction, their comparative safety has not been evaluated in a randomized clinical trial.
Objective: To determine whether the choice between cefepime and piperacillin-tazobactam affects the risks of acute kidney injury or neurological dysfunction.
Design, setting, and participants: The Antibiotic Choice on Renal Outcomes (ACORN) randomized clinical trial compared cefepime vs piperacillin-tazobactam in adults for whom a clinician initiated an order for antipseudomonal antibiotics within 12 hours of presentation to the hospital in the emergency department or medical intensive care unit at an academic medical center in the US between November 10, 2021, and October 7, 2022. The final date of follow-up was November 4, 2022.
Interventions: Patients were randomized in a 1:1 ratio to cefepime or piperacillin-tazobactam.
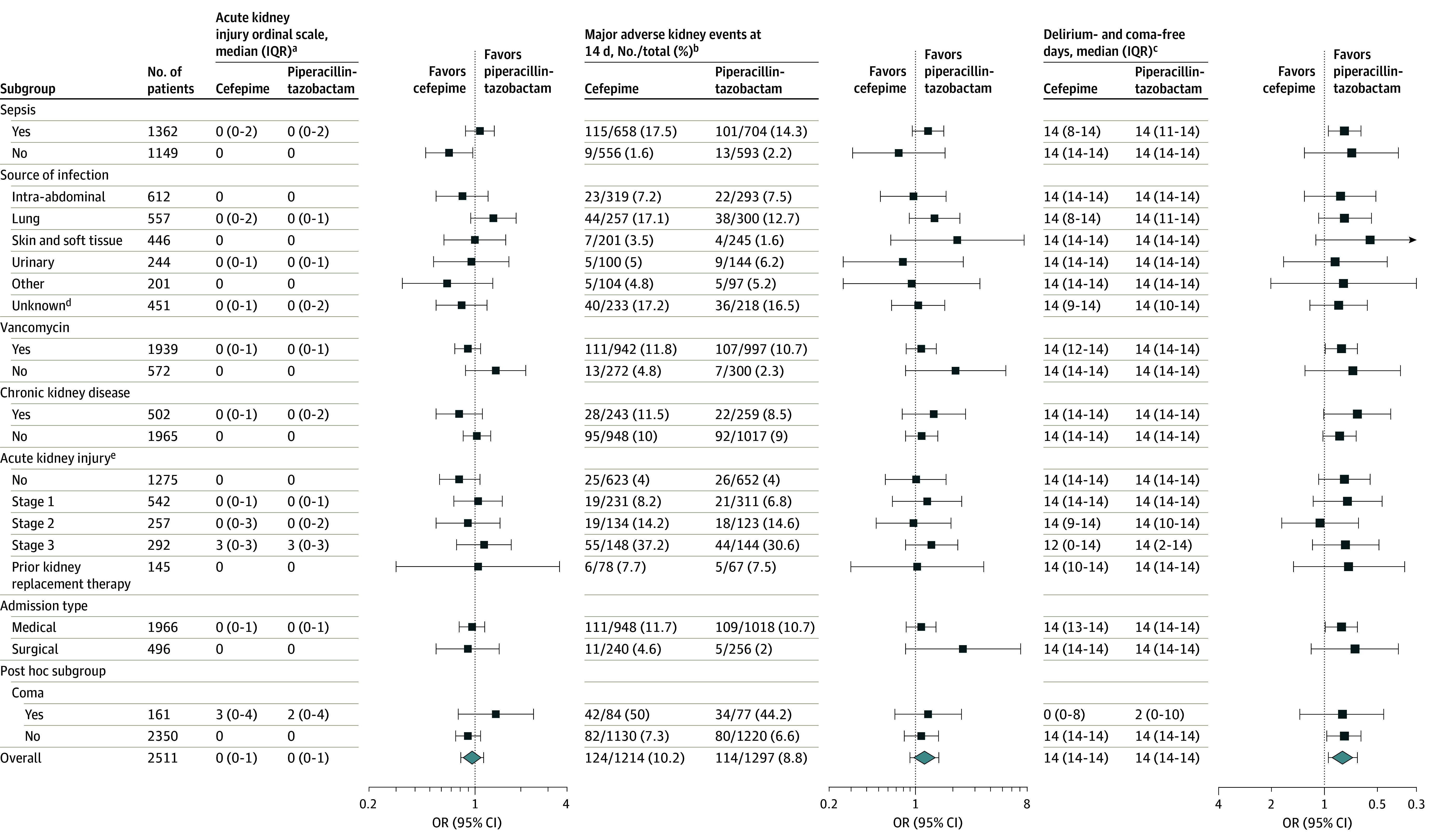
Main outcomes and measures: The primary outcome was the highest stage of acute kidney injury or death by day 14, measured on a 5-level ordinal scale ranging from no acute kidney injury to death. The 2 secondary outcomes were the incidence of major adverse kidney events at day 14 and the number of days alive and free of delirium and coma within 14 days.
Results: There were 2511 patients included in the primary analysis (median age, 58 years [IQR, 43-69 years]; 42.7% were female; 16.3% were Non-Hispanic Black; 5.4% were Hispanic; 94.7% were enrolled in the emergency department; and 77.2% were receiving vancomycin at enrollment). The highest stage of acute kidney injury or death was not significantly different between the cefepime group and the piperacillin-tazobactam group; there were 85 patients (n = 1214; 7.0%) in the cefepime group with stage 3 acute kidney injury and 92 (7.6%) who died vs 97 patients (n = 1297; 7.5%) in the piperacillin-tazobactam group with stage 3 acute kidney injury and 78 (6.0%) who died (odds ratio, 0.95 [95% CI, 0.80 to 1.13], P = .56). The incidence of major adverse kidney events at day 14 did not differ between groups (124 patients [10.2%] in the cefepime group vs 114 patients [8.8%] in the piperacillin-tazobactam group; absolute difference, 1.4% [95% CI, -1.0% to 3.8%]). Patients in the cefepime group experienced fewer days alive and free of delirium and coma within 14 days (mean [SD], 11.9 [4.6] days vs 12.2 [4.3] days in the piperacillin-tazobactam group; odds ratio, 0.79 [95% CI, 0.65 to 0.95]).
Conclusions and relevance: Among hospitalized adults in this randomized clinical trial, treatment with piperacillin-tazobactam did not increase the incidence of acute kidney injury or death. Treatment with cefepime resulted in more neurological dysfunction.
Trial registration: ClinicalTrials.gov Identifier: NCT05094154.
Conflict of interest statement
Figures


Comment in
-
Acute Kidney Injury With Empirical Antibiotics for Sepsis.JAMA. 2023 Oct 24;330(16):1531-1533. doi: 10.1001/jama.2023.18591. JAMA. 2023. PMID: 37837650 No abstract available.
-
Cefepime vs Piperacillin-Tazobactam for Acute Infection in Hospitalized Adults.JAMA. 2024 Feb 27;331(8):708. doi: 10.1001/jama.2023.27900. JAMA. 2024. PMID: 38411649 No abstract available.
-
Cefepime vs Piperacillin-Tazobactam for Acute Infection in Hospitalized Adults.JAMA. 2024 Feb 27;331(8):707-708. doi: 10.1001/jama.2023.27897. JAMA. 2024. PMID: 38411650 No abstract available.
-
Cefepime vs Piperacillin-Tazobactam for Acute Infection in Hospitalized Adults.JAMA. 2024 Feb 27;331(8):708-709. doi: 10.1001/jama.2023.27894. JAMA. 2024. PMID: 38411651 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1 RR024975/RR/NCRR NIH HHS/United States
- R01 HL164909/HL/NHLBI NIH HHS/United States
- R35 GM145375/GM/NIGMS NIH HHS/United States
- K23 HL143053/HL/NHLBI NIH HHS/United States
- U24 TR001608/TR/NCATS NIH HHS/United States
- UL1 TR002243/TR/NCATS NIH HHS/United States
- R18 HS026616/HS/AHRQ HHS/United States
- R01 HL161635/HL/NHLBI NIH HHS/United States
- U24 TR004437/TR/NCATS NIH HHS/United States
- R18 HS025910/HS/AHRQ HHS/United States
- OT2 HL156812/HL/NHLBI NIH HHS/United States
- R18 HS026158/HS/AHRQ HHS/United States
- K23 HL153584/HL/NHLBI NIH HHS/United States
- R33 HL155810/HL/NHLBI NIH HHS/United States
- P30 DK114809/DK/NIDDK NIH HHS/United States
- T32 HL087738/HL/NHLBI NIH HHS/United States
- U01 HL168478/HL/NHLBI NIH HHS/United States
