Lumped-parameter model as a non-invasive tool to assess coronary blood flow in AAOCA patients
- PMID: 37838795
- PMCID: PMC10576762
- DOI: 10.1038/s41598-023-44568-8
Lumped-parameter model as a non-invasive tool to assess coronary blood flow in AAOCA patients
Abstract
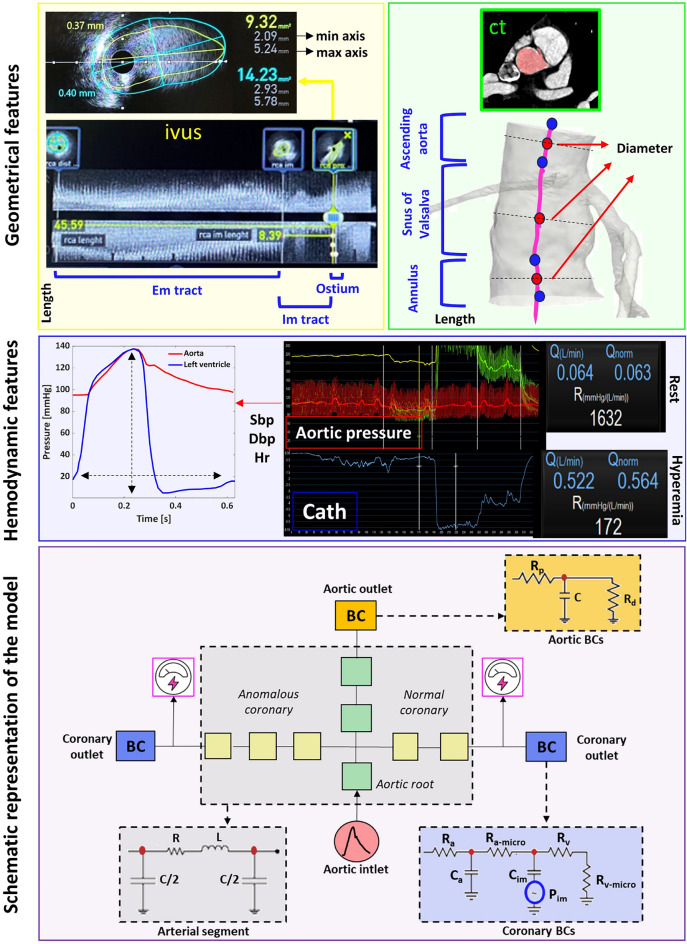
Anomalous aortic origin of the coronary artery (AAOCA) is a rare disease associated with sudden cardiac death, usually related to physical effort in young people. Clinical routine tests fail to assess the ischemic risk, calling for novel diagnostic approaches. To this aim, some recent studies propose to assess the coronary blood flow (CBF) in AAOCA by computational simulations but they are limited by the use of data from literature retrieved from normal subjects. To overcome this limitation and obtain a reliable assessment of CBF, we developed a fully patient-specific lumped parameter model based on clinical imaging and in-vivo data retrieved during invasive coronary functional assessment of subjects with AAOCA. In such a way, we can estimate the CBF replicating the two hemodynamic conditions in-vivo analyzed. The model can mimic the effective coronary behavior with high accuracy and could be a valuable tool to quantify CBF in AAOCA. It represents the first step required to move toward a future clinical application with the aim of improving patient care. The study was registered at Clinicaltrial.gov with (ID: NCT05159791, date 2021-12-16).
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures