

Impact of ventilation strategies on pulmonary and cardiovascular complications in patients undergoing general anaesthesia for elective surgery: a systematic review and meta-analysis
- PMID: 37839932
- PMCID: PMC10687618
- DOI: 10.1016/j.bja.2023.09.011
Impact of ventilation strategies on pulmonary and cardiovascular complications in patients undergoing general anaesthesia for elective surgery: a systematic review and meta-analysis
Abstract
Background: Many RCTs have evaluated the influence of intraoperative tidal volume (tV), PEEP, and driving pressure on the occurrence of postoperative pulmonary complications, cardiovascular complications, and mortality in adult patients. Our meta-analysis aimed to investigate the association between tV, PEEP, and driving pressure and the above-mentioned outcomes.
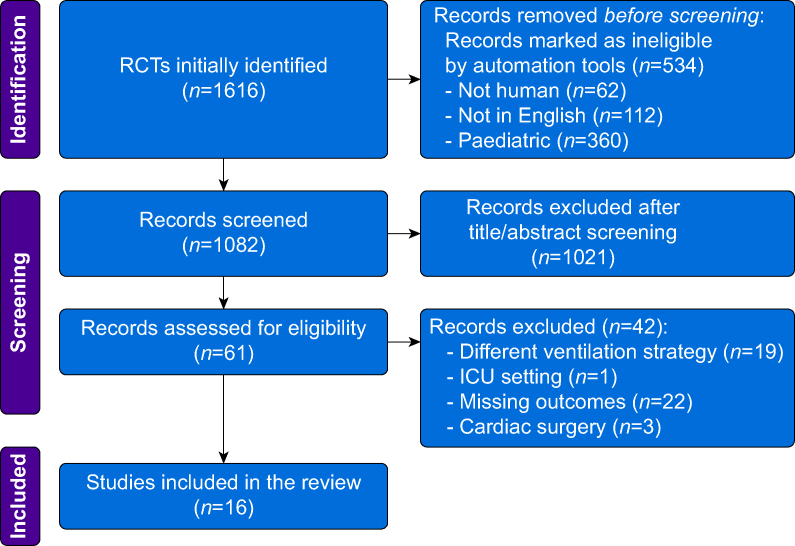
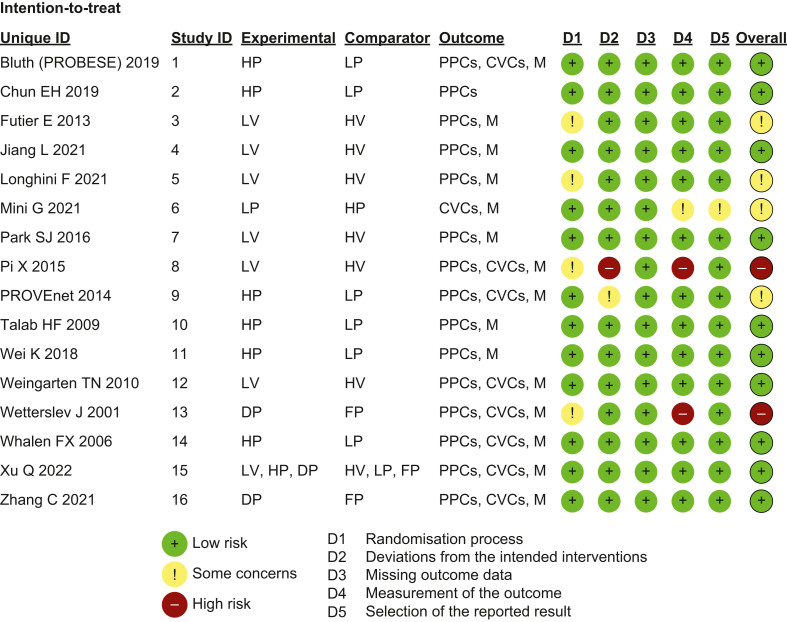
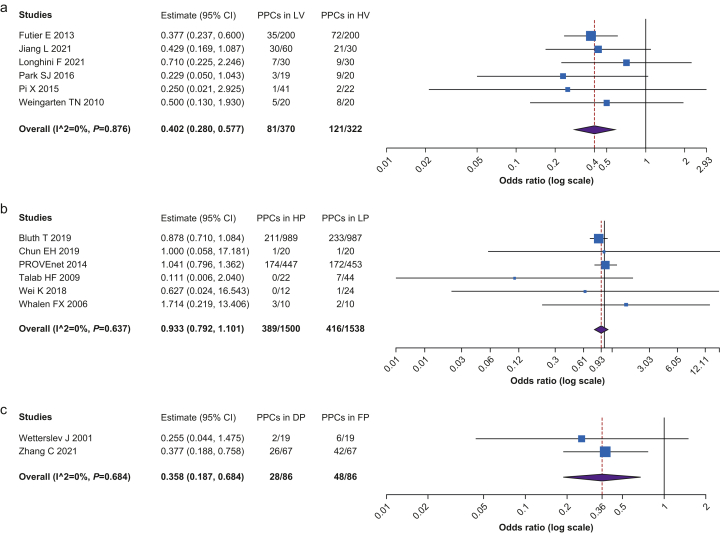
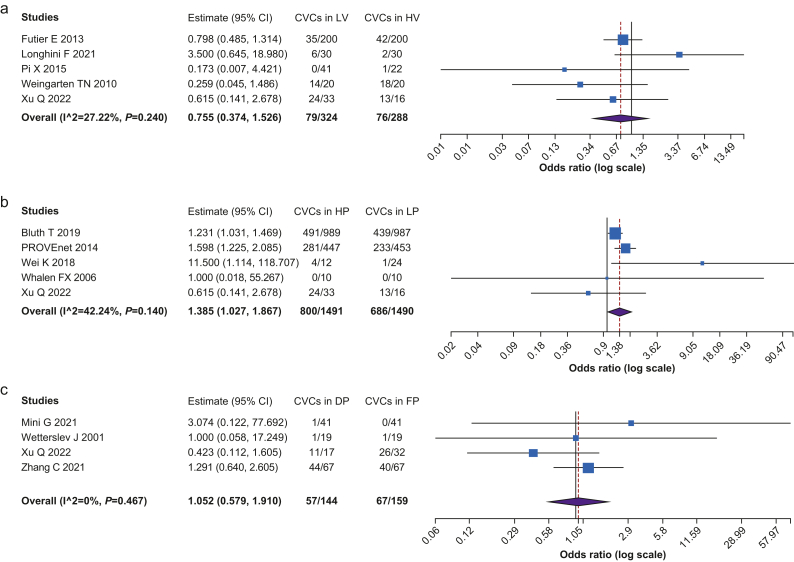
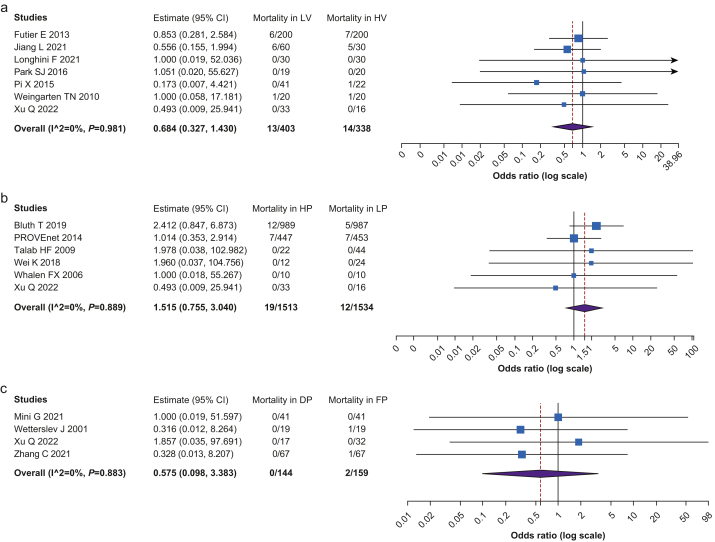
Methods: We conducted a systematic review and meta-analysis of RCTs from inception to May 19, 2022. The primary outcome was the incidence of postoperative pulmonary complications; the secondary outcomes were intraoperative cardiovascular complications and 30-day mortality. Primary and secondary outcomes were evaluated stratifying patients in the following groups: (1) low tV (LV, tV 6-8 ml kg-1 and PEEP ≥5 cm H2O) vs high tV (HV, tV >8 ml kg-1 and PEEP=0 cm H2O); (2) higher PEEP (HP, ≥6 cm H2O) vs lower PEEP (LP, <6 cm H2O); and (3) driving pressure-guided PEEP (DP) vs fixed PEEP (FP).
Results: We included 16 RCTs with a total sample size of 4993. The incidence of postoperative pulmonary complications was lower in patients treated with LV than with HV (OR=0.402, CI 0.280-0.577, P<0.001) and lower in DP than in FP group (OR=0.358, CI 0.187-0.684, P=0.002). Postoperative pulmonary complications did not differ between HP and LP groups; the incidence of intraoperative cardiovascular complications was higher in HP group (OR=1.385, CI 1.027-1.867, P=0.002). The 30-day mortality was not influenced by the ventilation strategy.
Conclusions: Optimal intraoperative mechanical ventilation is unclear; however, our meta-analysis showed that low tidal volume and driving pressure-guided PEEP strategies were associated with a reduction in postoperative pulmonary complications.
Keywords: driving pressure; general anaesthesia; positive end-expiratory pressure; postoperative pulmonary complications; ventilation strategy.
Copyright © 2023 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Intraoperative use of low volume ventilation to decrease postoperative mortality, mechanical ventilation, lengths of stay and lung injury in adults without acute lung injury.Cochrane Database Syst Rev. 2018 Jul 9;7(7):CD011151. doi: 10.1002/14651858.CD011151.pub3. Cochrane Database Syst Rev. 2018. PMID: 29985541 Free PMC article.
-
Positive end-expiratory pressure (PEEP) during anaesthesia for the prevention of mortality and postoperative pulmonary complications.Cochrane Database Syst Rev. 2010 Sep 8;(9):CD007922. doi: 10.1002/14651858.CD007922.pub2. Cochrane Database Syst Rev. 2010. Update in: Cochrane Database Syst Rev. 2014 Jun 12;(6):CD007922. doi: 10.1002/14651858.CD007922.pub3. PMID: 20824871 Updated.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Intra-operative ventilation strategies and their impact on clinical outcomes: a systematic review and network meta-analysis of randomised trials.Anaesthesia. 2025 Aug;80(8):973-987. doi: 10.1111/anae.16600. Epub 2025 Mar 25. Anaesthesia. 2025. PMID: 40133080 Free PMC article.
-
Low Tidal Volume versus Non-Volume-Limited Strategies for Patients with Acute Respiratory Distress Syndrome. A Systematic Review and Meta-Analysis.Ann Am Thorac Soc. 2017 Oct;14(Supplement_4):S271-S279. doi: 10.1513/AnnalsATS.201704-337OT. Ann Am Thorac Soc. 2017. PMID: 28846440
Cited by
-
Local anaesthesia with conscious sedation in parotid gland tumour resection: a retrospective review.BMC Oral Health. 2024 Dec 21;24(1):1531. doi: 10.1186/s12903-024-05318-y. BMC Oral Health. 2024. PMID: 39709417 Free PMC article.
-
Driving pressure: A useful tool for reducing postoperative pulmonary complications.World J Crit Care Med. 2024 Sep 9;13(3):96214. doi: 10.5492/wjccm.v13.i3.96214. eCollection 2024 Sep 9. World J Crit Care Med. 2024. PMID: 39253315 Free PMC article.
-
PEEP on postoperative complications: not to fast.J Anesth. 2024 Aug;38(4):573-574. doi: 10.1007/s00540-023-03299-w. Epub 2023 Dec 20. J Anesth. 2024. PMID: 38117328 No abstract available.
-
Effects of lung protection ventilation strategies on postoperative pulmonary complications after noncardiac surgery: a network meta-analysis of randomized controlled trials.BMC Anesthesiol. 2024 Sep 28;24(1):346. doi: 10.1186/s12871-024-02737-w. BMC Anesthesiol. 2024. PMID: 39342110 Free PMC article.
-
Impact of a positive end-expiratory pressure on oxygenation, respiratory compliance, and hemodynamics in obese patients undergoing laparoscopic surgery in reverse Trendelenburg position: a systematic review and meta-analysis of randomized controlled trials.BMC Anesthesiol. 2025 Feb 7;25(1):61. doi: 10.1186/s12871-025-02933-2. BMC Anesthesiol. 2025. PMID: 39915702 Free PMC article.
References
-
- Weiser T.G., Regenbogen S.E., Thompson K.D., et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 2008;372:139–144. - PubMed
-
- Serpa Neto A., Cardoso S.O., Manetta J.A., et al. Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome. JAMA. 2012;308:1651–1659. - PubMed
-
- Imai Y., Parodo J., Kajikawa O., et al. Injurious mechanical ventilation and end-organ epithelial cell apoptosis and organ dysfunction in an experimental model of acute respiratory distress syndrome. JAMA. 2003;289:2104–2112. - PubMed
-
- Lellouche F., Dionne S., Simard S., Bussières J., Dagenais F. High tidal volumes in mechanically ventilated patients increase organ dysfunction after cardiac surgery. Anesthesiology. 2012;116:1072–1082. - PubMed
-
- Futier E., Constantin J.-M., Paugam-Burtz C., et al. A Trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med. 2013;369:428–437. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
