

Impact of ventilation strategies on pulmonary and cardiovascular complications in patients undergoing general anaesthesia for elective surgery: a systematic review and meta-analysis
- PMID: 37839932
- PMCID: PMC10687618
- DOI: 10.1016/j.bja.2023.09.011
Impact of ventilation strategies on pulmonary and cardiovascular complications in patients undergoing general anaesthesia for elective surgery: a systematic review and meta-analysis
Abstract
Background: Many RCTs have evaluated the influence of intraoperative tidal volume (tV), PEEP, and driving pressure on the occurrence of postoperative pulmonary complications, cardiovascular complications, and mortality in adult patients. Our meta-analysis aimed to investigate the association between tV, PEEP, and driving pressure and the above-mentioned outcomes.
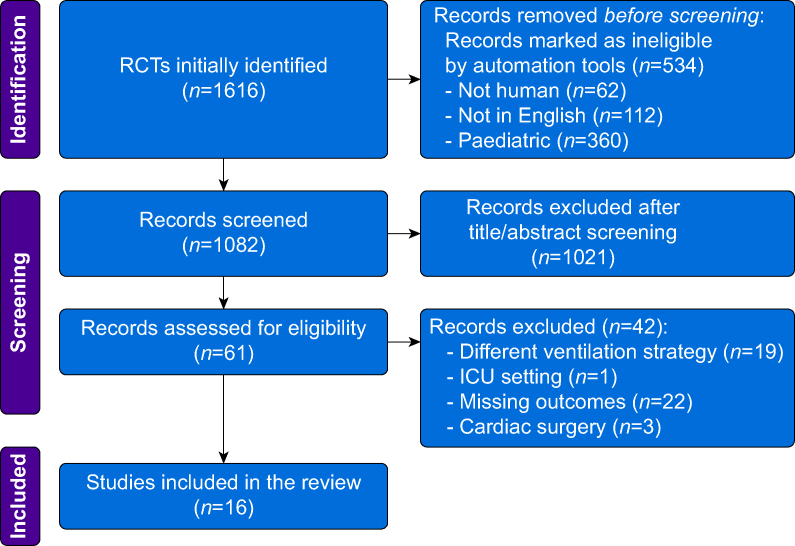
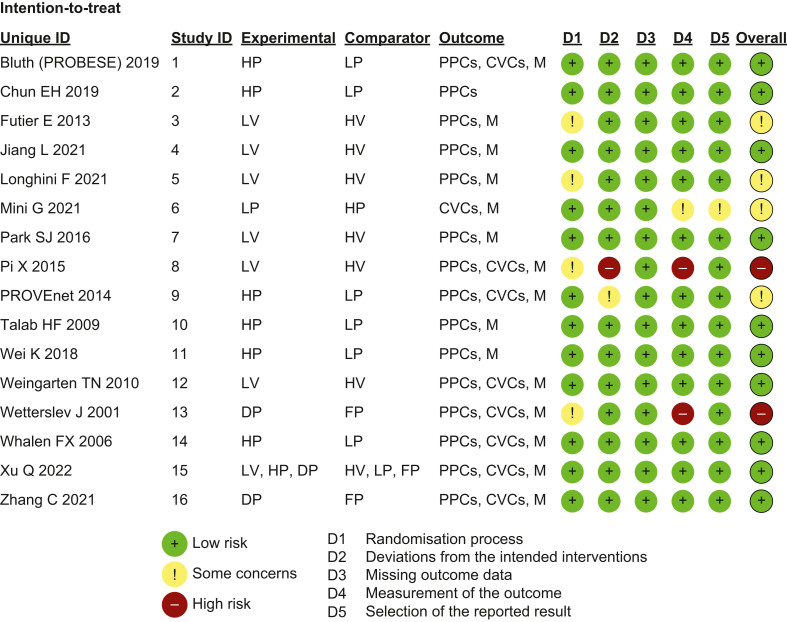
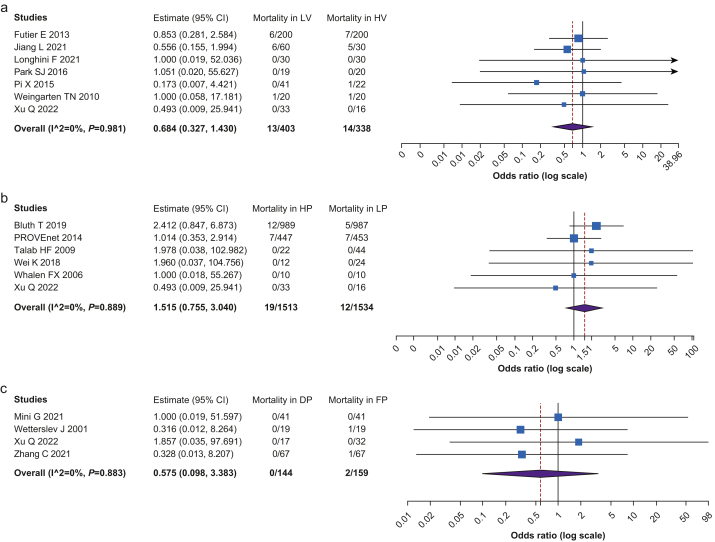
Methods: We conducted a systematic review and meta-analysis of RCTs from inception to May 19, 2022. The primary outcome was the incidence of postoperative pulmonary complications; the secondary outcomes were intraoperative cardiovascular complications and 30-day mortality. Primary and secondary outcomes were evaluated stratifying patients in the following groups: (1) low tV (LV, tV 6-8 ml kg-1 and PEEP ≥5 cm H2O) vs high tV (HV, tV >8 ml kg-1 and PEEP=0 cm H2O); (2) higher PEEP (HP, ≥6 cm H2O) vs lower PEEP (LP, <6 cm H2O); and (3) driving pressure-guided PEEP (DP) vs fixed PEEP (FP).
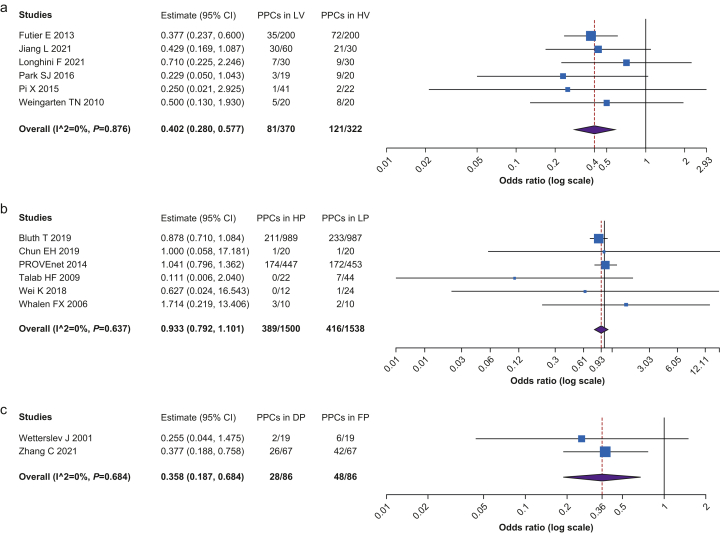
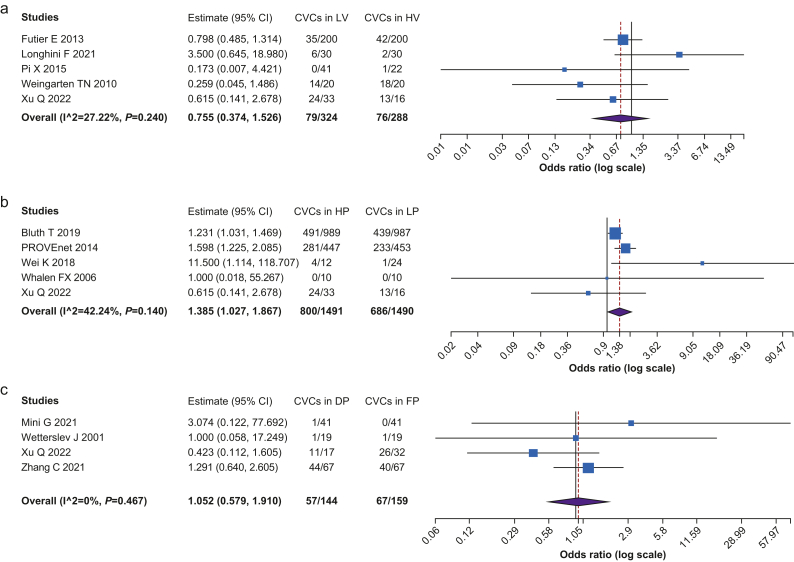
Results: We included 16 RCTs with a total sample size of 4993. The incidence of postoperative pulmonary complications was lower in patients treated with LV than with HV (OR=0.402, CI 0.280-0.577, P<0.001) and lower in DP than in FP group (OR=0.358, CI 0.187-0.684, P=0.002). Postoperative pulmonary complications did not differ between HP and LP groups; the incidence of intraoperative cardiovascular complications was higher in HP group (OR=1.385, CI 1.027-1.867, P=0.002). The 30-day mortality was not influenced by the ventilation strategy.
Conclusions: Optimal intraoperative mechanical ventilation is unclear; however, our meta-analysis showed that low tidal volume and driving pressure-guided PEEP strategies were associated with a reduction in postoperative pulmonary complications.
Keywords: driving pressure; general anaesthesia; positive end-expiratory pressure; postoperative pulmonary complications; ventilation strategy.
Copyright © 2023 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Weiser T.G., Regenbogen S.E., Thompson K.D., et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 2008;372:139–144. - PubMed
-
- Serpa Neto A., Cardoso S.O., Manetta J.A., et al. Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome. JAMA. 2012;308:1651–1659. - PubMed
-
- Imai Y., Parodo J., Kajikawa O., et al. Injurious mechanical ventilation and end-organ epithelial cell apoptosis and organ dysfunction in an experimental model of acute respiratory distress syndrome. JAMA. 2003;289:2104–2112. - PubMed
-
- Lellouche F., Dionne S., Simard S., Bussières J., Dagenais F. High tidal volumes in mechanically ventilated patients increase organ dysfunction after cardiac surgery. Anesthesiology. 2012;116:1072–1082. - PubMed
-
- Futier E., Constantin J.-M., Paugam-Burtz C., et al. A Trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med. 2013;369:428–437. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
