

Tirzepatide after intensive lifestyle intervention in adults with overweight or obesity: the SURMOUNT-3 phase 3 trial
- PMID: 37840095
- PMCID: PMC10667099
- DOI: 10.1038/s41591-023-02597-w
Tirzepatide after intensive lifestyle intervention in adults with overweight or obesity: the SURMOUNT-3 phase 3 trial
Erratum in
-
Author Correction: Tirzepatide after intensive lifestyle intervention in adults with overweight or obesity: the SURMOUNT-3 phase 3 trial.Nat Med. 2024 Jun;30(6):1784. doi: 10.1038/s41591-024-02883-1. Nat Med. 2024. PMID: 38409593 Free PMC article. No abstract available.
Abstract
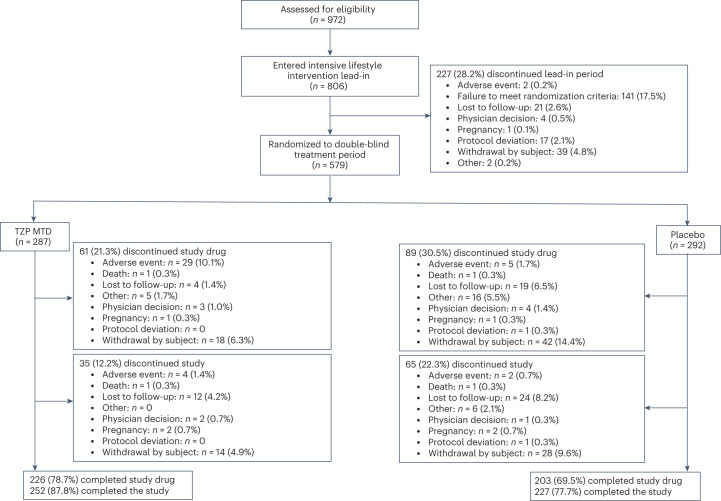
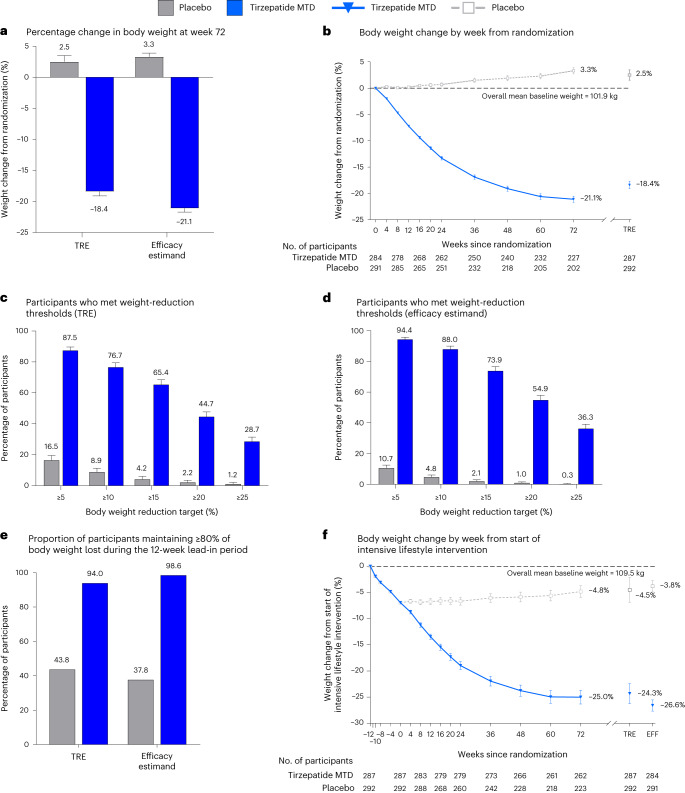
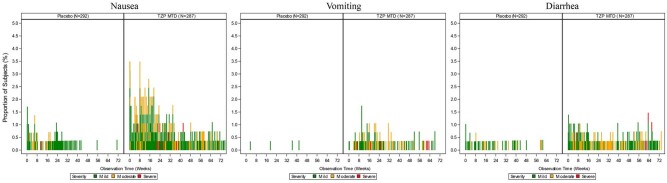
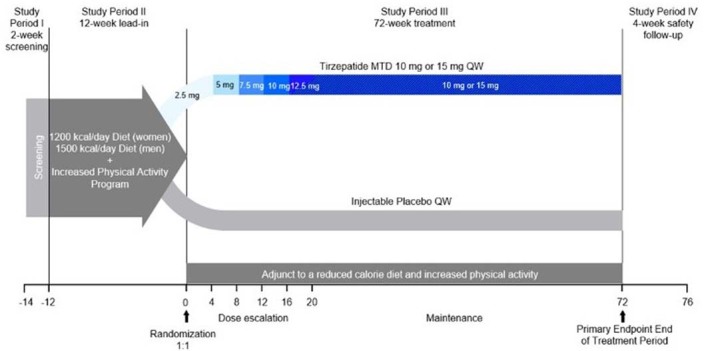
The effects of tirzepatide, a glucose-dependent insulinotropic polypeptide and glucagon-like peptide-1 receptor agonist, on weight reduction after successful intensive lifestyle intervention are unknown. This double-blind, placebo-controlled trial randomized (1:1) adults with body mass index ≥30 or ≥27 kg/m2 and at least one obesity-related complication (excluding diabetes), who achieved ≥5.0% weight reduction after a 12-week intensive lifestyle intervention, to tirzepatide maximum tolerated dose (10 or 15 mg) or placebo once weekly for 72 weeks (n = 579). The treatment regimen estimand assessed effects regardless of treatment adherence in the intention-to-treat population. The coprimary endpoint of additional mean per cent weight change from randomization to week 72 was met with changes of -18.4% (standard error (s.e.) 0.7) with tirzepatide and 2.5% (s.e. 1.0) with placebo (estimated treatment difference -20.8 percentage points (95% confidence interval (CI) -23.2%, -18.5%; P < 0.001). The coprimary endpoint of the percentage of participants achieving additional weight reduction ≥5% was met with 87.5% (s.e. 2.2) with tirzepatide and 16.5% (s.e. 3.0) with placebo achieving this threshold (odds ratio 34.6%; 95% CI 19.2%, 62.6%; P < 0.001). The most common adverse events with tirzepatide were gastrointestinal, with most being mild to moderate in severity. Tirzepatide provided substantial additional reduction in body weight in participants who had achieved ≥5.0% weight reduction with intensive lifestyle intervention. ClinicalTrials.gov registration: NCT04657016 .
© 2023. The Author(s).
Conflict of interest statement
T.A.W. reports grants or contracts from Novo Nordisk, Epitomee Medical Co. and Eli Lilly and Company; and service on Scientific Advisory Boards for Novo Nordisk and WW. A.M.C. reports grants or contracts from National Institutes of Health, WW International, Inc, The Edna G. Kynett Memorial Foundation, Novo Nordisk and Epitomee Medical; consulting fees from Eli Lilly and Company and Boehringer Ingelheim; and payment or honoraria for presentation and travel/meeting support from the Obesity Medicine Association. S.M. reports grants or contracts from Boehringer Ingelheim, Rhythm Pharmaceuticals and Novo Nordisk; consulting fees from Novo Nordisk, Rhythm Pharmaceuticals and Eli Lilly and Company; payment or honoraria from Columbia University Medical Center, Boston Obesity Course in Obesity medicine and Medical College of Wisconsin; and participation on Advisory Boards for Novo Nordisk and Eli Lilly and Company. R.K. reports participation on a Data Safety Monitoring Board or Advisory Board for Eli Lilly and Company, Novo Nordisk and Boehringer Ingelheim. J.A. reports grants or contracts from Nestle Healthcare Nutrition, Eli Lilly and Company, Boehringer Ingelheim, Epitomee, Inc., UnitedHealth Group R&D, KVK Tech and WW; consulting fees from Nestle Healthcare Nutrition, Eli Lilly and Company, Optum Labs R&D, Novo Nordisk, Spokes Health, Inc., Intuitive, Regeneron, Brightseed, Level2 and WW; receipt of equipment, materials, drugs, medical writing, gifts or other services from KVK Tech, WW and Nestle Healthcare Nutrition; and is President Elect of The Obesity Society and an Executive Board Member of the American Society for Nutrition Foundation. G.S. reports consulting fees from Rhythm Pharmaceuticals, Novo Nordisk and Eli Lilly and Company; and speaker’s bureau from Novo Nordisk. B.H. reports payment or honoraria from Eli Lilly and Company, Novo Nordisk, Merck S.A., Astra Zeneca and Abbott Nutrition; travel/meeting support from Novo Nordisk; participation on a Data Safety Monitoring Board or Advisory Board for Eli Lilly, Novo Nordisk and Merck S.A; receipt of equipment, materials, drugs, medical writing, gifts or other services from Eli Lilly and Company and Novo Nordisk; and is President of the Brazilian Association of Obesity and a Member of Board of Trustees of World Obesity Federation representing Latin America. S.Z., J.C., M.C.B., N.N.A. and T.F. are employees and shareholders of Eli Lilly and Company.
Figures
References
-
- World Health Organization. Obesity and Overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed 8 August 2023).
-
- Jensen MD, et al. Guidelines (2013) for the management of overweight and obesity in adults. Obesity. 2014;22:i–xvi. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
