

Mortality and immune-related adverse events after immune checkpoint inhibitor initiation for cancer among patients with pre-existing rheumatoid arthritis: a retrospective, comparative, cohort study
- PMID: 37841635
- PMCID: PMC10571093
- DOI: 10.1016/s2665-9913(23)00064-4
Mortality and immune-related adverse events after immune checkpoint inhibitor initiation for cancer among patients with pre-existing rheumatoid arthritis: a retrospective, comparative, cohort study
Erratum in
-
Correction to Lancet Rheumatol 2023; 5: e274-83.Lancet Rheumatol. 2023 May;5(5):e251. doi: 10.1016/S2665-9913(23)00103-0. Lancet Rheumatol. 2023. PMID: 38251586 No abstract available.
Abstract
Background: Patients with pre-existing rheumatoid arthritis initiating immune checkpoint inhibitors for cancer might be at risk of increased mortality, rheumatoid arthritis flares, and other immune-related adverse events (AEs). We aimed to determine whether pre-existing rheumatoid arthritis was associated with higher mortality and immune-related AE risk in patients treated with immune checkpoint inhibitors.
Methods: This retrospective, comparative cohort study was conducted at the Mass General Brigham Integrated Health Care System and the Dana-Farber Cancer Institute in Boston (MA, USA). We searched data repositories to identify all individuals who initiated immune checkpoint inhibitors from April 1, 2011, to April 21, 2021. Patients with pre-existing rheumatoid arthritis had to meet the 2010 American College of Rheumatology-European Alliance of Associations for Rheumatology (ACR-EULAR) criteria. For each pre-existing rheumatoid arthritis case, we matched up to three non-rheumatoid arthritis comparators at the index date of immune checkpoint inhibitor initiation by sex (recorded as male or female), calendar year, immune checkpoint inhibitor target, and cancer type and stage. The coprimary outcomes were time from index date to death and time to the first immune-related AE, measured using an adjusted Cox proportional hazards model. Deaths were identified by medical record and obituary review. Rheumatoid arthritis flares and immune-related AE presence, type, and severity were determined by medical record review.
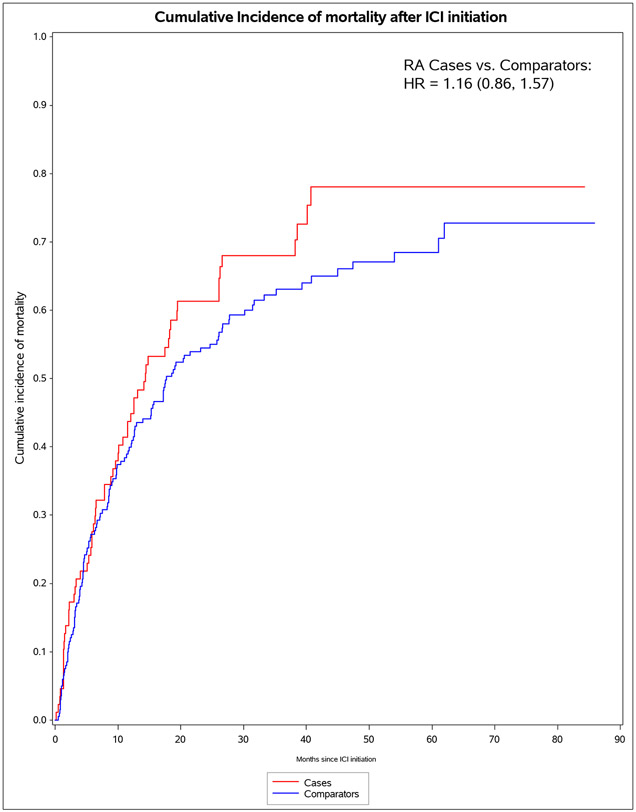
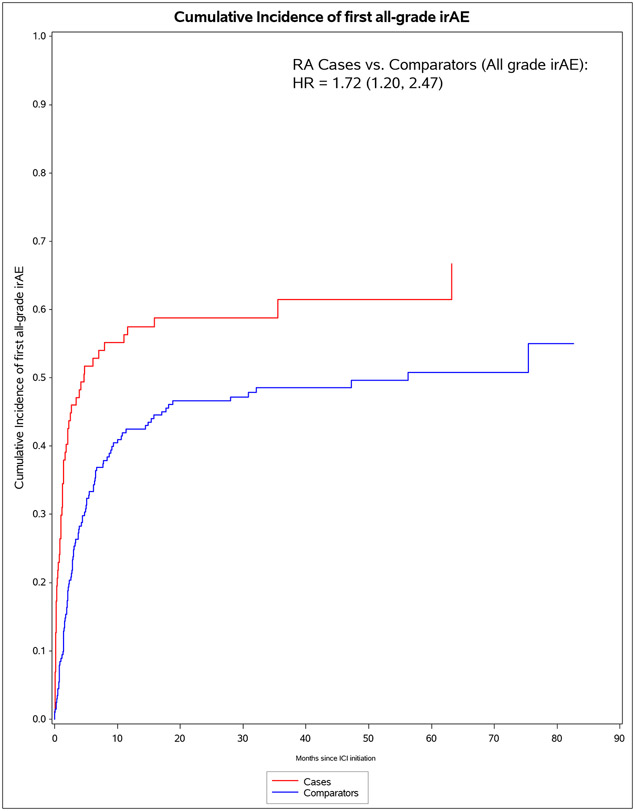
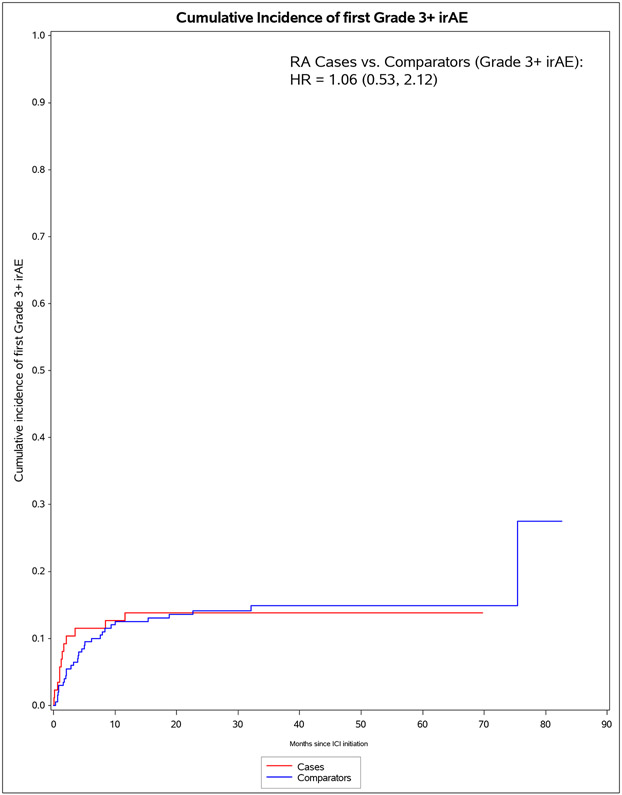
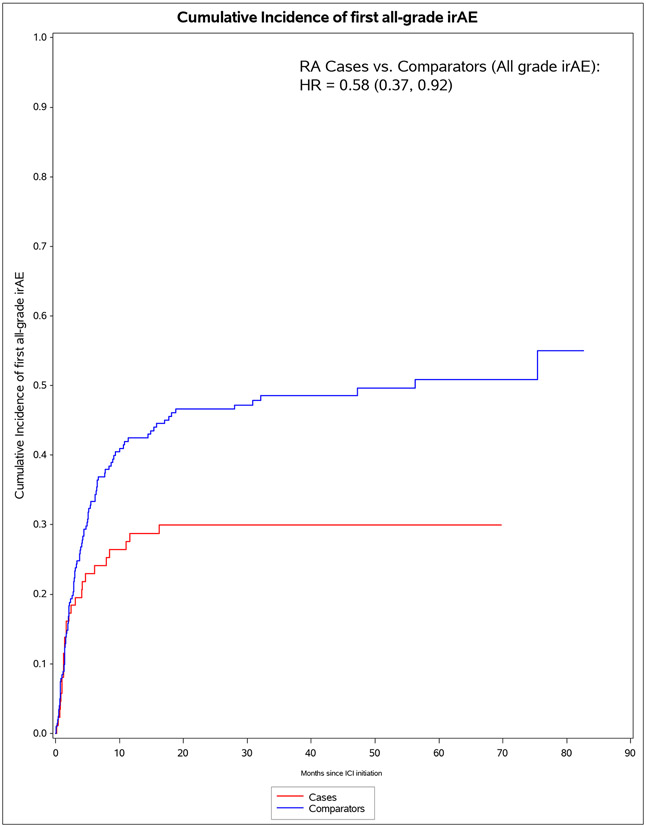
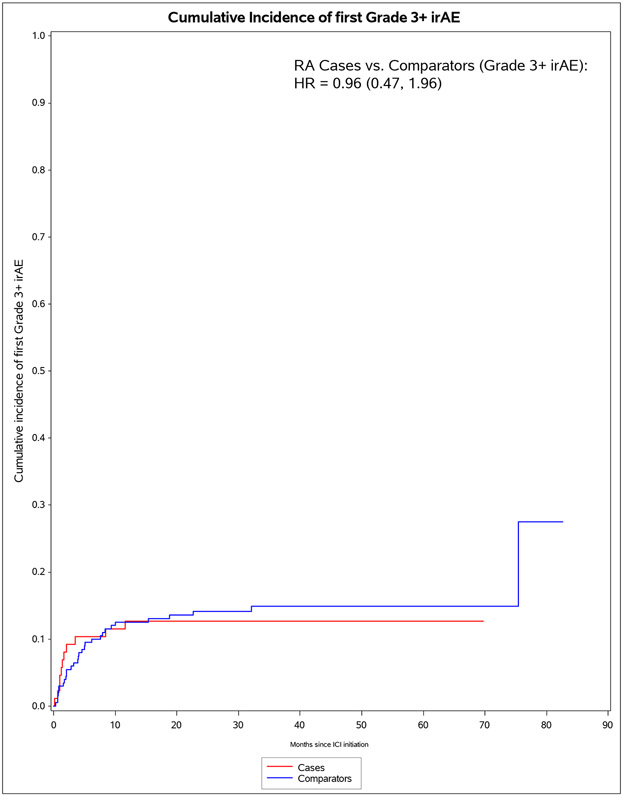
Findings: We identified 11 901 patients who initiated immune checkpoint inhibitors for cancer treatment between April 1, 2011, and April 21, 2021; of those, 101 met the 2010 ACR-EULAR criteria for rheumatoid arthritis. We successfully matched 87 patients with pre-existing rheumatoid arthritis to 203 non-rheumatoid arthritis comparators. The median age was 71·2 years (IQR 63·2-77·1). 178 (61%) of 290 participants were female, 112 (39%) were male and 268 (92%) participants were White. PD-1 was the most common immune checkpoint inhibitor target (80 [92%] of 87 patients with rheumatoid arthritis vs 188 [93%] of 203 comparators). Lung cancer was the most common cancer type (43 [49%] vs 114 [56%]), followed by melanoma (21 [24%] vs 50 [25%]). 60 (69%) patients with rheumatoid arthritis versus 127 (63%) comparators died (adjusted hazard ratio [HR] of 1·16 [95% CI 0·86-1·57]; p=0·34). 53 (61%) patients with rheumatoid arthritis versus 99 (49%) comparators had any all-grade immune-related AE (adjusted HR 1·72 [95% CI 1·20-2·47]; p=0·0032). There were two (1%) grade 5 immune-related AEs (deaths) due to myocarditis, both in the comparator group. Rheumatoid arthritis flares occurred in 42 (48%) patients with rheumatoid arthritis, and inflammatory arthritis occurred in 14 (7%) comparators (p<0·0001). Those with rheumatoid arthritis were less likely to have rash or dermatitis (five [6%] vs 28 [14%]; p=0·048), endocrinopathy (two [2%] vs 22 [11%]; p=0·0078), colitis or enteritis (six [7%] vs 28 [14%] comparators; p=0·094), and hepatitis (three [3%] vs 19 [9%]; p=0·043).
Interpretation: Patients with pre-existing rheumatoid arthritis initiating immune checkpoint inhibitors had similar risk of mortality and severe immune-related AEs as matched comparators. Although patients with pre-existing rheumatoid arthritis were more likely to have immune-related AEs, this finding was mostly due to mild rheumatoid arthritis flares. These results suggest that this patient population can safely receive immune checkpoint inhibitors for cancer treatment.
Funding: None.
Conflict of interest statement
Declaration of interests: Dr. Yoshida has received consulting fees from OM1, Inc. at the time of this work and is now employed by and owns stock options from OM1, Inc unrelated to this work. Dr. Shadick is supported by Mallinckrodt, Lilly, BMS, Amgen, Abbvie, and Aqtual unrelated to this work. Dr. LeBoeuf receives consulting fees from Bayer, Seattle Genetics, Sanofi, Silverback, and Synox Therapeutics unrelated to this work. Dr. Buchbinder has received a research grant from Genentech and has participated on advisory boards for Merck, Bristol Myers Squibb, and Novartis unrelated to this work. Dr. Gedmintas has received honoraria for invited lectures for the Harvard Continuing Medical Education programs Intensive Review of Internal Medicine and Innovations and New Practices in Internal Medicine (not sponsored by for-profit institutions). Dr. Gravallese receives royalties from UpToDate and the Rheumatology textbook (published by Elsevier), has received honoraria for scientific lectures at academic institutions/meetings (none for industry or for-profit institutions) and the American College of Rheumatology (serving on task forces for COVID treatment and vaccine guidelines), has received reimbursement for travel to academic institutions and meetings hosted by the American College of Rheumatology, and has received partial salary support serving as president-elect and president of the American College of Rheumatology and as an Associate Editor for the New England Journal of Medicine. Dr. Sparks has received research support from Bristol Myers Squibb and performed consultancy for AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Gilead, Inova Diagnostics, Janssen, Optum, and Pfizer unrelated to this work. All other authors report no conflicts of interest.
Figures
Comment in
-
Reconciling immunotherapy and autoimmunity: not for the faint of heart.Lancet Rheumatol. 2023 May;5(5):e243-e245. doi: 10.1016/S2665-9913(23)00059-0. Epub 2023 Mar 27. Lancet Rheumatol. 2023. PMID: 38251584 No abstract available.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous