

Post-viral olfactory loss and parosmia
- PMID: 37841969
- PMCID: PMC10568123
- DOI: 10.1136/bmjmed-2022-000382
Post-viral olfactory loss and parosmia
Abstract
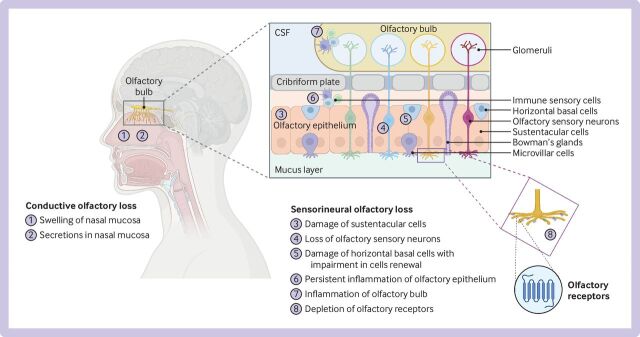
The emergence of SARS-CoV-2 has brought olfactory dysfunction to the forefront of public awareness, because up to half of infected individuals could develop olfactory dysfunction. Loss of smell-which can be partial or total-in itself is debilitating, but the distortion of sense of smell (parosmia) that can occur as a consequence of a viral upper respiratory tract infection (either alongside a reduction in sense of smell or as a solo symptom) can be very distressing for patients. Incidence of olfactory loss after SARS-CoV-2 infection has been estimated by meta-analysis to be around 50%, with more than one in three who will subsequently report parosmia. While early loss of sense of smell is thought to be due to infection of the supporting cells of the olfactory epithelium, the underlying mechanisms of persistant loss and parosmia remain less clear. Depletion of olfactory sensory neurones, chronic inflammatory infiltrates, and downregulation of receptor expression are thought to contribute. There are few effective therapeutic options, so support and olfactory training are essential. Further research is required before strong recommendations can be made to support treatment with steroids, supplements, or interventions applied topically or injected into the olfactory epithelium in terms of improving recovery of quantitative olfactory function. It is not yet known whether these treatments will also achieve comparable improvements in parosmia. This article aims to contextualise parosmia in the setting of post-viral olfactory dysfunction, explore some of the putative molecular mechanisms, and review some of the treatment options available.
Keywords: epidemiology; pathology, surgical; pharmacology, clinical; physiology.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: We have read and understood the BMJ policy on declaration of interests and declare the following interests: none.
Figures
Similar articles
-
Parosmia is Associated with Relevant Olfactory Recovery After Olfactory Training.Laryngoscope. 2021 Mar;131(3):618-623. doi: 10.1002/lary.29277. Epub 2020 Nov 19. Laryngoscope. 2021. PMID: 33210732
-
Clinical Features of Parosmia Associated With COVID-19 Infection.Laryngoscope. 2022 Mar;132(3):633-639. doi: 10.1002/lary.29982. Epub 2021 Dec 13. Laryngoscope. 2022. PMID: 34870334 Free PMC article.
-
Proof-of-concept: SCENTinel 1.1 rapidly discriminates COVID-19 related olfactory disorders.medRxiv [Preprint]. 2022 Nov 8:2022.03.23.22272807. doi: 10.1101/2022.03.23.22272807. medRxiv. 2022. Update in: Chem Senses. 2023 Jan 1;48:bjad002. doi: 10.1093/chemse/bjad002. PMID: 35350197 Free PMC article. Updated. Preprint.
-
Parosmia and Phantosmia: Managing Quality Disorders.Curr Otorhinolaryngol Rep. 2023;11(1):19-26. doi: 10.1007/s40136-023-00441-w. Epub 2023 Jan 27. Curr Otorhinolaryngol Rep. 2023. PMID: 36721659 Free PMC article. Review.
-
Anosmia: an evolution of our understanding of its importance in COVID-19 and what questions remain to be answered.Eur Arch Otorhinolaryngol. 2021 Jul;278(7):2187-2191. doi: 10.1007/s00405-020-06285-0. Epub 2020 Sep 9. Eur Arch Otorhinolaryngol. 2021. PMID: 32909060 Free PMC article. Review.
Cited by
-
Long-term olfactory loss post-COVID-19: Pathobiology and potential therapeutic strategies.World J Otorhinolaryngol Head Neck Surg. 2024 Mar 21;10(2):148-155. doi: 10.1002/wjo2.165. eCollection 2024 Jun. World J Otorhinolaryngol Head Neck Surg. 2024. PMID: 38855286 Free PMC article. Review.
-
Postviral olfactory dysfunction.CMAJ. 2025 Feb 9;197(5):E131. doi: 10.1503/cmaj.241377. CMAJ. 2025. PMID: 39929487 Free PMC article. No abstract available.
-
Scent of COVID-19: Whole-Genome Sequencing Analysis Reveals the Role of ACE2, IFI44, and NDUFAF4 in Long-Lasting Olfactory Dysfunction.Life (Basel). 2025 Jan 5;15(1):56. doi: 10.3390/life15010056. Life (Basel). 2025. PMID: 39859996 Free PMC article.
-
Viral Etiologies and Histopathological Features of Olfactory Dysfunction: A Systematic Review.Health Sci Rep. 2025 Jun 18;8(6):e70917. doi: 10.1002/hsr2.70917. eCollection 2025 Jun. Health Sci Rep. 2025. PMID: 40535522 Free PMC article. Review.
-
Structures and functions of the normal and injured human olfactory epithelium.Front Neural Circuits. 2024 Jun 6;18:1406218. doi: 10.3389/fncir.2024.1406218. eCollection 2024. Front Neural Circuits. 2024. PMID: 38903957 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous