

End organ perfusion and pediatric microcirculation assessment
- PMID: 37842022
- PMCID: PMC10576530
- DOI: 10.3389/fped.2023.1123405
End organ perfusion and pediatric microcirculation assessment
Abstract
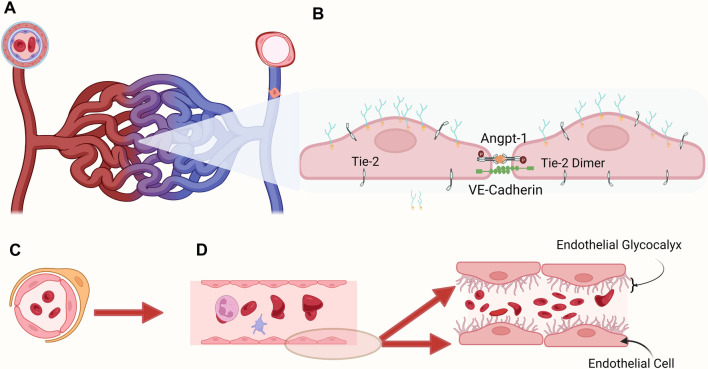
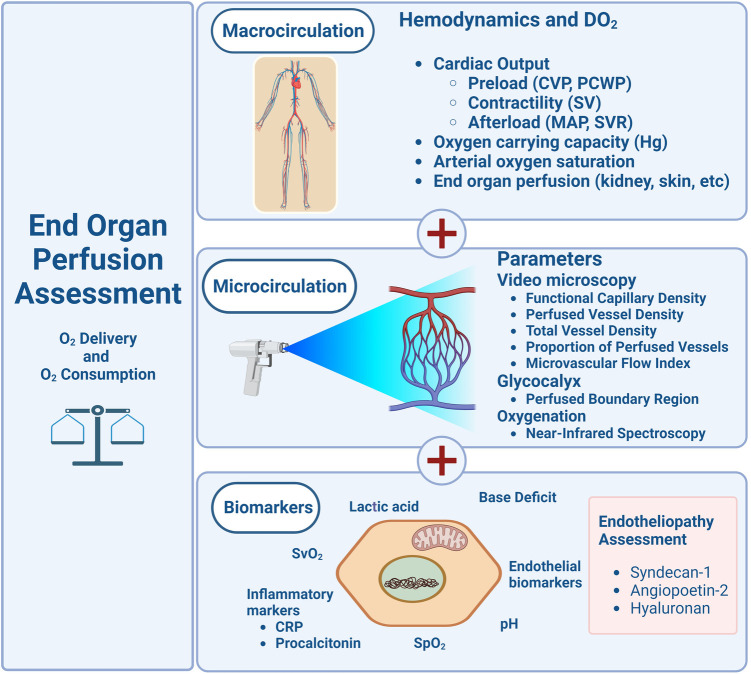
Cardiovascular instability and reduced oxygenation are regular perioperative critical events associated with anesthesia requiring intervention in neonates and young infants. This review article addresses the current modalities of assessing this population's adequate end-organ perfusion in the perioperative period. Assuring adequate tissue oxygenation in critically ill infants is based on parameters that measure acceptable macrocirculatory hemodynamic parameters such as vital signs (mean arterial blood pressure, heart rate, urinary output) and chemical parameters (lactic acidosis, mixed venous oxygen saturation, base deficit). Microcirculation assessment represents a promising candidate for assessing and improving hemodynamic management strategies in perioperative and critically ill populations. Evaluation of the functional state of the microcirculation can parallel improvement in tissue perfusion, a term coined as "hemodynamic coherence". Less information is available to assess microcirculatory disturbances related to higher mortality risk in critically ill adults and pediatric patients with septic shock. Techniques for measuring microcirculation have substantially improved in the past decade and have evolved from methods that are limited in scope, such as velocity-based laser Doppler and near-infrared spectroscopy, to handheld vital microscopy (HVM), also referred to as videomicroscopy. Available technologies to assess microcirculation include sublingual incident dark field (IDF) and sublingual sidestream dark field (SDF) devices. This chapter addresses (1) the physiological basis of microcirculation and its relevance to the neonatal and pediatric populations, (2) the pathophysiology associated with altered microcirculation and endothelium, and (3) the current literature reviewing modalities to detect and quantify the presence of microcirculatory alterations.
Keywords: children; critically ill; hemodynamic; microcirculation; neonate; videomicroscopy.
© 2023 Arteaga and Crow.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Assessing the Microcirculation With Handheld Vital Microscopy in Critically Ill Neonates and Children: Evolution of the Technique and Its Potential for Critical Care.Front Pediatr. 2019 Jul 9;7:273. doi: 10.3389/fped.2019.00273. eCollection 2019. Front Pediatr. 2019. PMID: 31338353 Free PMC article. Review.
-
Recent advances in bedside microcirculation assessment in critically ill patients.Rev Bras Ter Intensiva. 2017 Apr-Jun;29(2):238-247. doi: 10.5935/0103-507X.20170033. Rev Bras Ter Intensiva. 2017. PMID: 28977264 Free PMC article. Review.
-
The response of the microcirculation to mechanical support of the heart in critical illness.Best Pract Res Clin Anaesthesiol. 2016 Dec;30(4):511-522. doi: 10.1016/j.bpa.2016.10.001. Epub 2016 Oct 27. Best Pract Res Clin Anaesthesiol. 2016. PMID: 27931654 Review.
-
Tissue perfusion and oxygenation to monitor fluid responsiveness in critically ill, septic patients after initial resuscitation: a prospective observational study.J Clin Monit Comput. 2015 Dec;29(6):707-12. doi: 10.1007/s10877-014-9653-8. Epub 2015 Jan 20. J Clin Monit Comput. 2015. PMID: 25599945 Free PMC article.
-
Monitoring the microcirculation in the critically ill patient: current methods and future approaches.Intensive Care Med. 2010 Nov;36(11):1813-25. doi: 10.1007/s00134-010-2005-3. Epub 2010 Aug 6. Intensive Care Med. 2010. PMID: 20689916 Review.
Cited by
-
Microcirculation, endothelium and glycocalyx changes associated with the use of milrinone in children with septic shock.Transl Pediatr. 2024 May 31;13(5):727-737. doi: 10.21037/tp-23-619. Epub 2024 May 27. Transl Pediatr. 2024. PMID: 38840690 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous