

Innovative Health and Social Integrated Care Model Effectiveness to Improve Quality Care for Chronic Patients: A Single Group Assignment Clinical Trial
- PMID: 37842263
- PMCID: PMC10573743
- DOI: 10.5334/ijic.6759
Innovative Health and Social Integrated Care Model Effectiveness to Improve Quality Care for Chronic Patients: A Single Group Assignment Clinical Trial
Abstract
Background: Patients with chronic disease have become one of the major challenges for health and social protection systems in developed countries. Integrated care models (ICM) have demonstrably improved the quality of care of chronic patients. However, new models of integration need further evaluation of its effectiveness and outcomes.
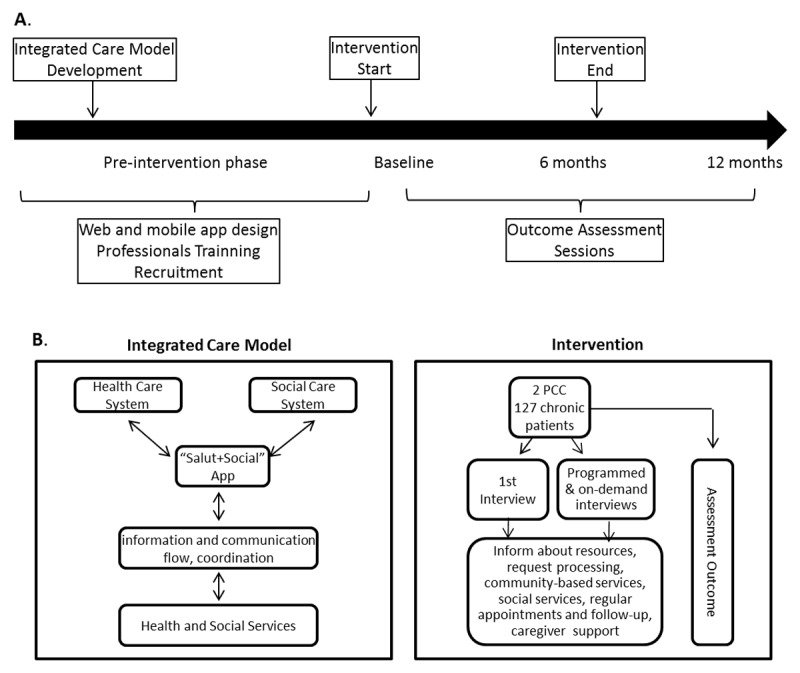
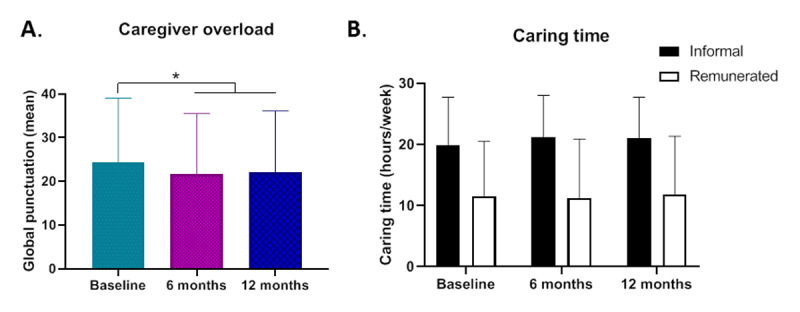
Methods: The ICM studied promoted coordination between the health and social sectors during a 6-month period, through an ad hoc developed application (app) that enabled a constant flow of communication between professionals from both sectors. Patients' quality of life, treatment adherence, chronic patient experience and caregiver overload were assessed by questionnaires at baseline, at the end of the intervention and 6 months post-intervention.
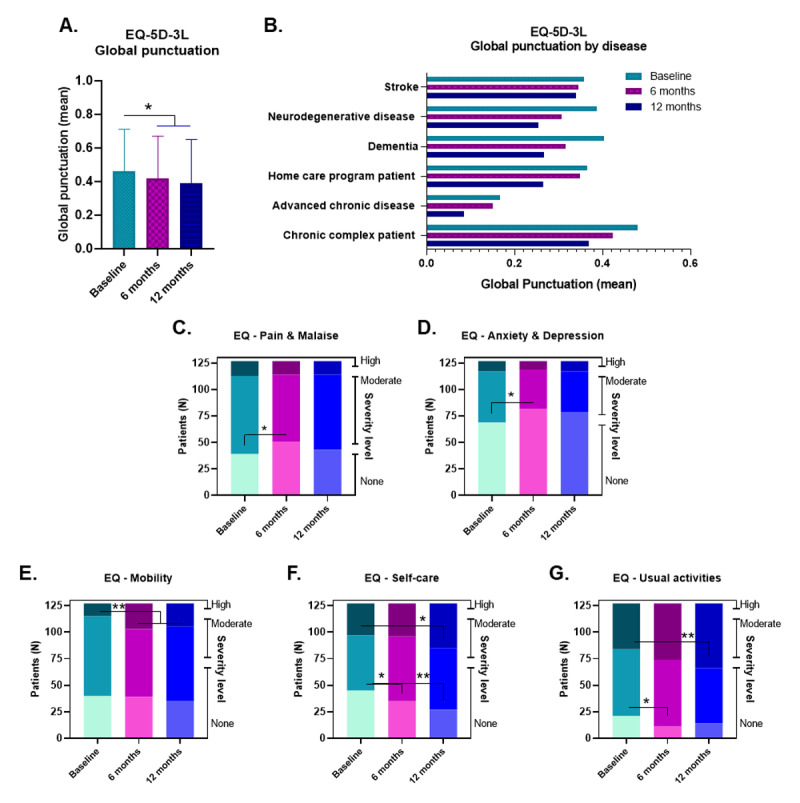
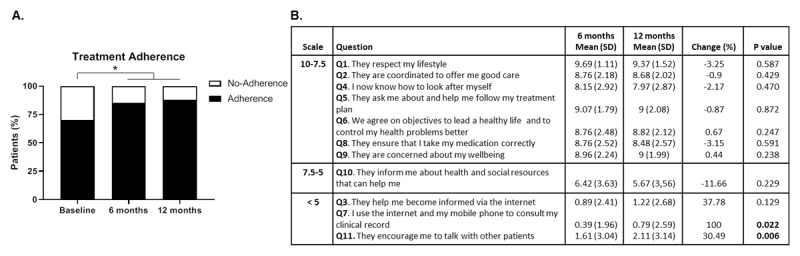
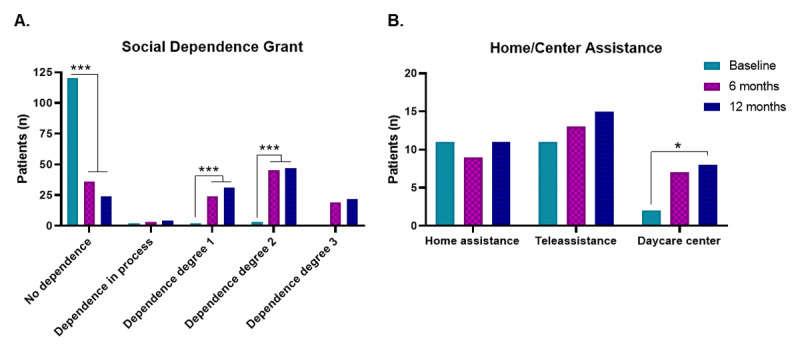
Results: The implementation of the new health and social ICM permitted new case detection and medical and social services offered to chronic patients. Furthermore, the quality of life and treatment adherence of patients and caregiver overload were significantly improved. These positive effects lasted at least 6 months after the intervention.
Conclusions: Integrated care may facilitate access to care services, increase perceived patient quality of life and treatment adherence. Enhanced access to medical and social services from complex chronic patients may have important implications for caregivers and the care systems who are struggling to adapt to an expanding demand.
Antecedents: Els pacients amb malalties cròniques representen un dels grans reptes per als sistemes de salut i protecció social als països desenvolupats. S’ha demostrat que l’atenció integrada millora la qualitat assistencial dels pacients crònics. Tanmateix, els resultats i l’efectivitat de nous models d’integració requereixen ser avaluats.
Metodologia: El model d’atenció integrada d’estudi va promoure la coordinació entre els sectors sanitari i social durant un període de 6 mesos mitjançant una aplicació (app) desenvolupada ad hoc que permetia un flux constant de comunicació entre professionals d’ambdós sectors. La qualitat de vida dels pacients, l’adherència al tractament, l’experiència del pacient i la sobrecàrrega del cuidador es van avaluar mitjançant qüestionaris a l’inici, al final de la intervenció i 6 mesos després de la intervenció.
Resultats: La implantació de l’atenció integrada social i sanitària va permetre la detecció de nous casos i un major accés dels pacients crònics als serveis mèdics i socials. A més, va millorar significativament la qualitat de vida i l’adherència al tractament dels pacients i la sobrecàrrega dels cuidadors. Aquests efectes positius van perdurar almenys 6 mesos després de la intervenció.
Conclusions: L’atenció integrada pot facilitar l’accés als serveis assistencials, augmentar la qualitat de vida percebuda dels pacients i l’adherència al tractament. L’accés millorat als serveis mèdics i socials dels pacients crònics complexos pot tenir implicacions importants per als cuidadors i els sistemes assistencials que lluiten per adaptar-se a una demanda creixent.
Keywords: chronic disease; implementation science; information and communication technology (ICT); integrated healthcare systems; quality of life.
Copyright: © 2023 The Author(s).
Conflict of interest statement
The authors have no competing interests to declare.
Figures
References
LinkOut - more resources
Full Text Sources
