

Insulin resistance and central obesity determine hepatic steatosis and explain cardiovascular risk in steatotic liver disease
- PMID: 37842290
- PMCID: PMC10570507
- DOI: 10.3389/fendo.2023.1244405
Insulin resistance and central obesity determine hepatic steatosis and explain cardiovascular risk in steatotic liver disease
Abstract
Background: Metabolic dysfunction-associated steatotic liver disease (MASLD) has recently been proposed to replace non-alcoholic fatty liver disease and focus on patients with progressive disease due to the presence of metabolic dysfunction. However, it is unclear whether the new definition actually identifies patients with hepatic steatosis at increased cardiovascular risk.
Methods: A total of 4,286 asymptomatic subjects from the SAKKOPI study aged 45-80 years undergoing screening colonoscopy were analyzed. Steatosis was diagnosed by abdominal ultrasound. MASLD was diagnosed according to the recent expert consensus. Insulin resistance was assessed by homeostasis model assessment-insulin resistance score (HOMA-IR) (cutoff: ≥2.5), subclinical inflammation was estimated by ferritin/CRP/uric acid, and cardiovascular risk was assessed using SCORE2/ASCVD.
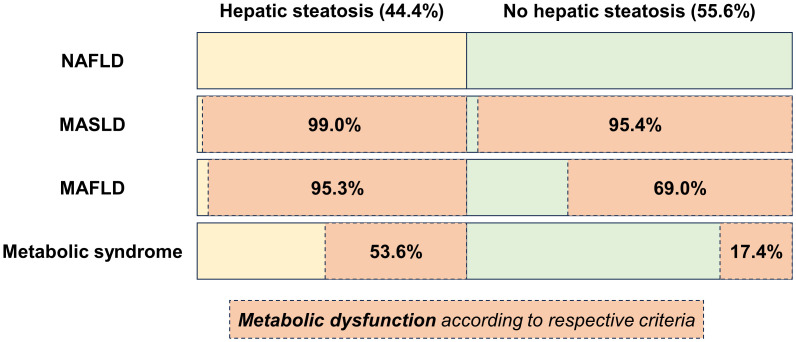
Results: Mean age was 59.4 ± 8.5 years, 51.6% were male; mean BMI was 27.0 ± 4.5 kg/m², 9.2% had type 2 diabetes mellitus. In total, 1,903 (44.4%) were diagnosed with hepatic steatosis and were characterized by more severe metabolic dysfunction including insulin resistance (47.1% vs. 12.2%, p < 0.001) and central obesity (waist circumference ≥102/88 cm, 71.8% vs. 37.1%, p < 0.001). This translated into higher (subclinical) inflammation (ferritin 153 vs. 95 mg/dL, p < 0.001, uric acid 6.3 mg/dL vs. 5.2 mg/dL, p < 0.001) and 10-year cardiovascular risk (SCORE2 7.8 points vs. 5.1 points, p < 0.001, ASCVD 17.9 points vs. 10.8 points, p < 0.001). 99.0% of subjects with steatosis met the MASLD definition, 95.4% met the MAFLD definition, and 53.6% met the definition of metabolic syndrome, while 95.4% of subjects without steatosis also met the MASLD criteria for metabolic dysfunction compared to 69.0% and 17.4% who met the MAFLD and metabolic syndrome criteria, respectively. Forward stepwise regression indicated that waist circumference, HOMA-IR, and triglycerides were most relevant in explaining the presence of hepatic steatosis across all subgroups of increasing metabolic dysfunction. At the same time, hepatic steatosis was not associated with cardiovascular risk in the overall cohort (SCORE2: B = 0.060, 95% CI: -0.193-0.314, and p = 0.642) and in patients with metabolic dysfunction after adjusting for age, sex, and these three metabolic dysfunction components.
Conclusion: Although hepatic steatosis is associated with increased central obesity and insulin resistance, metabolic dysfunction per se rather than hepatic steatosis explains cardiovascular risk in these patients.
Keywords: MASLD; NAFLD; SCORE2; insulin resistance; metabolic syndrome; steatotic liver disease.
Copyright © 2023 Semmler, Balcar, Wernly, Völkerer, Semmler, Hauptmann, Wernly, Aigner, Niederseer and Datz.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Mantovani A, Csermely A, Petracca G, Beatrice G, Corey KE, Simon TG, et al. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: an updated systematic review and meta-analysis. Lancet Gastroenterol hepatol (2021) 6(11):903–13. doi: 10.1016/S2468-1253(21)00308-3 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous