

International Physical Activity Questionnaire Short Form and accelerometer-assessed physical activity: concurrent validity using six cut-points in HF patients
- PMID: 37842962
- PMCID: PMC10804186
- DOI: 10.1002/ehf2.14514
International Physical Activity Questionnaire Short Form and accelerometer-assessed physical activity: concurrent validity using six cut-points in HF patients
Abstract
Aims: Physical activity (PA) is an important target for improving clinical outcomes in heart failure (HF) patients. Nonetheless, assessing the daily PA profile in this population is a challenging task, traditionally performed using self-report questionnaires such as the International PA Questionnaire Short Form (IPAQ-SF). This study aimed to evaluate the concurrent validity of the IPAQ-SF and accelerometer-assessed PA using six published cut-points in patients with HF and reduced or mildly reduced ejection fraction.
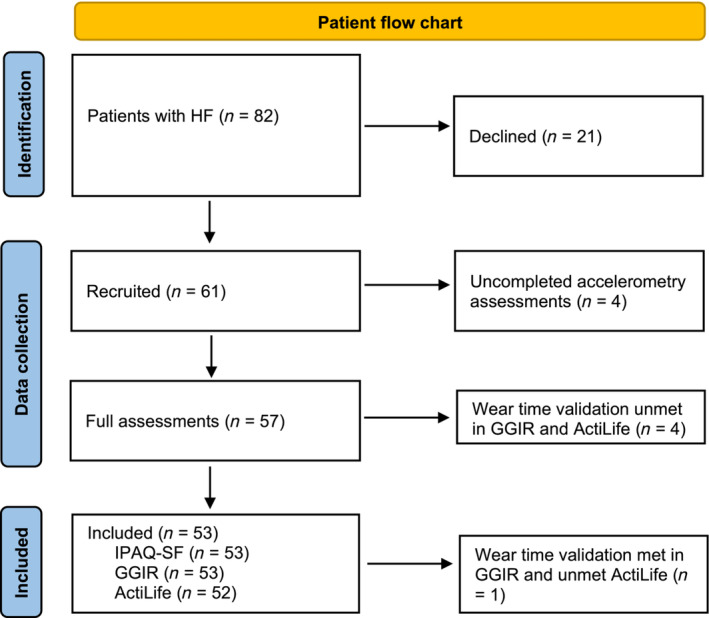
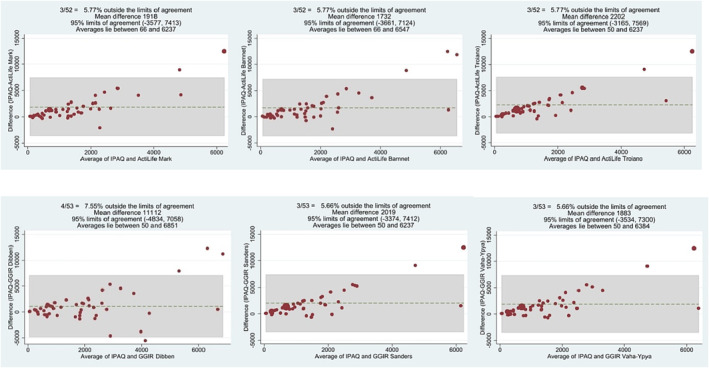
Methods and results: The concordance between the IPAQ-SF and a hip-worn accelerometer regarding daily time spent performing moderate to vigorous PA in bouts of at least 10 min was assessed in 53 participants for seven consecutive days using six different cut-points (Barnett, Dibben, Mark, Sanders, Troiano, and Vaha-Ypya). Spearman's correlation and Bland-Altman plots were used to evaluate concurrent validity between methods. Regressions were used to study the association between patient variables, wear protocol (waking hour or 24 h), and absolute bias. The kappa index was used to evaluate the concordance between IPAQ-SF and accelerometry for classifying patients as active or non-active. All analyses were re-run using non-bouted metrics to investigate the effect of bouted versus non-bouted analysis. The IPAQ-SF and accelerometry showed low to negligible correlation (ρ = 0.12 to 0.37), depending on the cut-point used. The regression analysis showed that the absolute bias was higher in participants following the waking-hour protocol at all cut-points except Dibben's (P ≤ 0.007). The concordance between the two methods to classify patients as active and non-active was low when using Mark (κ = 0.23) and Barnett (κ = 0.34) cut-points and poor for the remaining cut-points (κ = 0.03 to 0.18). The results of the sensitivity analysis showed negligible to low correlation using non-bouted metrics (ρ = 0.27 to 0.33).
Conclusions: Moderate to vigorous PA measures using IPAQ-SF and accelerometers are not equivalent, and we do not encourage researchers to use IPAQ-SF alone when assessing PA in HF patients. Moreover, applying personalized collection and processing criteria is important when assessing PA in HF patients. We recommend following the 24 h protocol and selecting cut-points calibrated in patients with cardiovascular diseases. Finally, it is necessary to develop a new tailored questionnaire that considers walking intensity and is adjusted to the current World Health Organisation recommendations, which use non-bouted metrics.
Keywords: Activity monitor; Agreement; Device-based measures; HF; MVPA; Self-reported measures.
© 2023 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Concurrent validity between self-reported International Physical Activity Questionnaire Short Form and Fibion accelerometer data among young adults in the UAE.Eur J Med Res. 2024 Aug 19;29(1):426. doi: 10.1186/s40001-024-01975-5. Eur J Med Res. 2024. PMID: 39155363 Free PMC article.
-
Reliability and concurrent validity of the International Physical Activity Questionnaire short form among pregnant women.BMC Sports Sci Med Rehabil. 2017 Mar 14;9:7. doi: 10.1186/s13102-017-0070-4. eCollection 2017. BMC Sports Sci Med Rehabil. 2017. PMID: 28316789 Free PMC article.
-
Concurrent validity of the International Physical Activity Questionnaire adapted for adults aged ≥ 80 years (IPAQ-E 80 +) - tested with accelerometer data from the SilverMONICA study.Gait Posture. 2022 Feb;92:135-143. doi: 10.1016/j.gaitpost.2021.11.019. Epub 2021 Nov 22. Gait Posture. 2022. PMID: 34847411
-
Advances in accelerometry for cardiovascular patients: a systematic review with practical recommendations.ESC Heart Fail. 2020 Oct;7(5):2021-2031. doi: 10.1002/ehf2.12781. Epub 2020 Jul 3. ESC Heart Fail. 2020. PMID: 32618431 Free PMC article.
-
The Physical Activity Assessment of Adults With Type 2 Diabetes Using Accelerometer-Based Cut Points: Scoping Review.Interact J Med Res. 2022 Sep 6;11(2):e34433. doi: 10.2196/34433. Interact J Med Res. 2022. PMID: 36066937 Free PMC article.
Cited by
-
The association of back pain with physical inactivity and hypothyroidism in pregnant women.J Back Musculoskelet Rehabil. 2024;37(6):1663-1671. doi: 10.3233/BMR-240086. J Back Musculoskelet Rehabil. 2024. PMID: 38968044 Free PMC article.
-
Ecological momentary assessment of physical and eating behaviours: The WEALTH feasibility and optimisation study with recommendations for large-scale data collection.PLoS One. 2025 Feb 11;20(2):e0318772. doi: 10.1371/journal.pone.0318772. eCollection 2025. PLoS One. 2025. PMID: 39932907 Free PMC article.
References
-
- Blasco‐Peris C, Fuertes‐Kenneally L, Vetrovsky T, Sarabia JM, Climent‐Paya V, Manresa‐Rocamora A. Effects of exergaming in patients with cardiovascular disease compared to conventional cardiac rehabilitation: A systematic review and meta‐analysis. Int J Environ Res Public Health 2022;19:3492. doi:10.3390/ijerph19063492 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
