

Transanal local excision versus intersphincteric resection for low rectal cancer with stage ypT0-1ycN0 after neoadjuvant chemoradiotherapy: an inverse probability weighting analysis for oncological and functional outcomes
- PMID: 37843558
- PMCID: PMC11796958
- DOI: 10.1007/s00432-023-05454-y
Transanal local excision versus intersphincteric resection for low rectal cancer with stage ypT0-1ycN0 after neoadjuvant chemoradiotherapy: an inverse probability weighting analysis for oncological and functional outcomes
Abstract
Objectives: This study aimed to compare the efficacy of local excision (LE) and intersphincteric resection (ISR) in patients with locally advanced rectal cancer who achieved a significant or complete pathological response following neoadjuvant chemoradiotherapy.
Methods: We performed a retrospective analysis of data from patients with stage ypT0-1ycN0 low rectal cancer after neoadjuvant chemoradiotherapy who underwent LE or ISR between June 2016 and June 2021. Baseline characteristics, short-term outcomes, long-term oncological outcomes, and functional outcomes, were compared between the two groups. To reduce the selection bias, inverse probability of treatment weighting (IPTW) was performed.
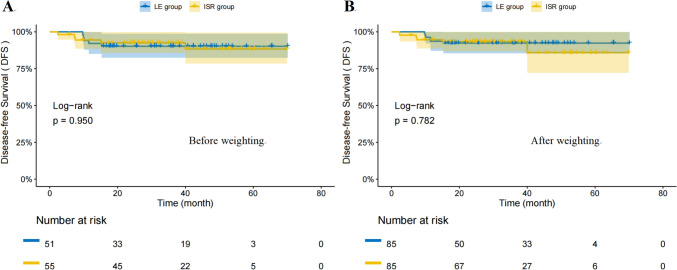
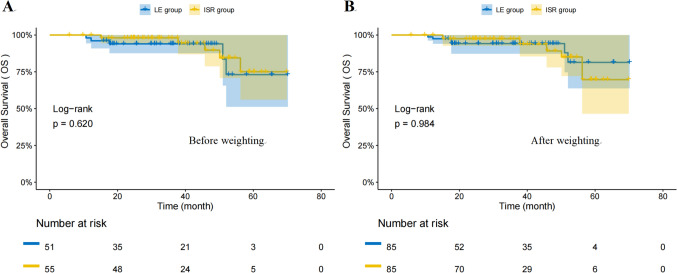
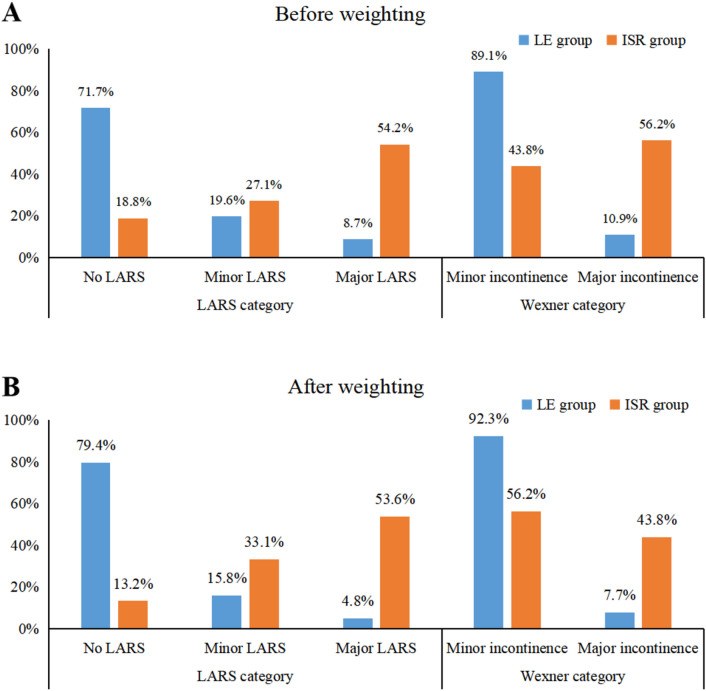
Results: This study included 106 patients (LE group: n = 51, ISR group: n = 55). There were significant differences in baseline characteristics between the two groups (P < 0.05). After IPTW, there were almost no significant differences in baseline data between the two groups. The LE group showed less postoperative complications and better function outcomes compared to the ISR group. The LE group had significantly lower rates of complications (13.7% vs. 36.4%, P = 0.014). There were no significant differences between the two groups in terms of long-term oncological outcomes.
Conclusions: For patients with locally advanced low rectal cancer achieving significant or complete pathological response after neoadjuvant therapy, both LE and ISR present comparable oncological outcomes. Yet, LE seems to show more advantages in terms of postoperative complications and functional outcomes. These findings offer important insights for surgical decision-making, emphasizing the necessity to consider both oncological and functional outcomes in selecting the optimal surgical approach.
Keywords: Intersphincteric resection; Local excision; Locally advanced rectal cancer; Neoadjuvant therapy; Outcomes.
© 2023. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Short-term outcomes of transanal endoscopic intersphincteric resection for locally advanced rectal cancer after neoadjuvant chemoradiotherapy: A single-center retrospective cohort study.Eur J Surg Oncol. 2025 Jul;51(7):109984. doi: 10.1016/j.ejso.2025.109984. Epub 2025 Mar 21. Eur J Surg Oncol. 2025. PMID: 40203672
-
Completion total mesorectal excision after neoadjuvant radiochemotherapy and local excision for rectal cancer.Colorectal Dis. 2024 Feb;26(2):281-289. doi: 10.1111/codi.16834. Epub 2023 Dec 22. Colorectal Dis. 2024. PMID: 38131642
-
Hysterectomy with radiotherapy or chemotherapy or both for women with locally advanced cervical cancer.Cochrane Database Syst Rev. 2015 Apr 7;(4):CD010260. doi: 10.1002/14651858.CD010260.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2022 Aug 22;8:CD010260. doi: 10.1002/14651858.CD010260.pub3. PMID: 25847525 Updated.
-
Oncologic outcomes of watch-and-wait strategy or surgery for low to intermediate rectal cancer in clinical complete remission after adjuvant chemotherapy: a systematic review and meta-analysis.Int J Colorectal Dis. 2023 Oct 3;38(1):246. doi: 10.1007/s00384-023-04534-2. Int J Colorectal Dis. 2023. PMID: 37787779
-
Outcomes of Distal Rectal Cancer Patients Who Did Not Qualify for Watch-and-Wait: Comparison of Intersphincteric Resection Versus Abdominoperineal Resection.Ann Surg Oncol. 2025 Jan;32(1):128-136. doi: 10.1245/s10434-024-16316-3. Epub 2024 Oct 12. Ann Surg Oncol. 2025. PMID: 39395915
Cited by
-
Predicting unplanned readmission due to cardiovascular disease in hospitalized patients with cancer: a machine learning approach.Sci Rep. 2023 Aug 18;13(1):13491. doi: 10.1038/s41598-023-40552-4. Sci Rep. 2023. PMID: 37596346 Free PMC article.
-
Therapeutic strategies for ypT1 rectal cancer after neoadjuvant chemoradiotherapy: a retrospective cohort study.Int J Colorectal Dis. 2024 Nov 26;39(1):189. doi: 10.1007/s00384-024-04764-y. Int J Colorectal Dis. 2024. PMID: 39592493 Free PMC article.
References
-
- Asoglu O, Bulut A, Aliyev V, Piozzi GN, Guven K, Bakır B, Goksel S (2022) Chemoradiation and consolidation chemotherapy for rectal cancer provides a high rate of organ preservation with a very good long-term oncological outcome: a single-center cohort series. World J Surg Oncol 20(1):358 - PMC - PubMed
-
- Battersby NJ, Juul T, Christensen P, Janjua AZ, Branagan G, Emmertsen KJ, Norton C, Hughes R, Laurberg S, Moran BJ (2016) Predicting the risk of bowel-related quality-of-life impairment after restorative resection for rectal cancer: a multicenter cross-sectional study. Dis Colon Rectum 59(4):270–280 - PubMed
-
- Chawla S, Katz AW, Rauh SM, Monson JR (2015) Can surgery be avoided after preoperative chemoradiation for rectal cancer in the era of organ preservation? Current review of literature. Am J Clin Oncol 38(5):534–540 - PubMed
MeSH terms
Grants and funding
- X-J-2018-004/Bethune Charitable Foundation
- 2020J011030, 2022J01753/Natural Science Foundation of Fujian Province
- 2020GGB022, 2020CXA025/Fujian Provincial Health Technology Project
- K99 CA252020/CA/NCI NIH HHS/United States
- Grant number: [2017]171/Construction Project of Fujian Province Minimally Invasive Medical Center
LinkOut - more resources
Full Text Sources
