

ECMO in trauma care: What you need to know
- PMID: 37843631
- PMCID: PMC12068791
- DOI: 10.1097/TA.0000000000004152
ECMO in trauma care: What you need to know
Abstract
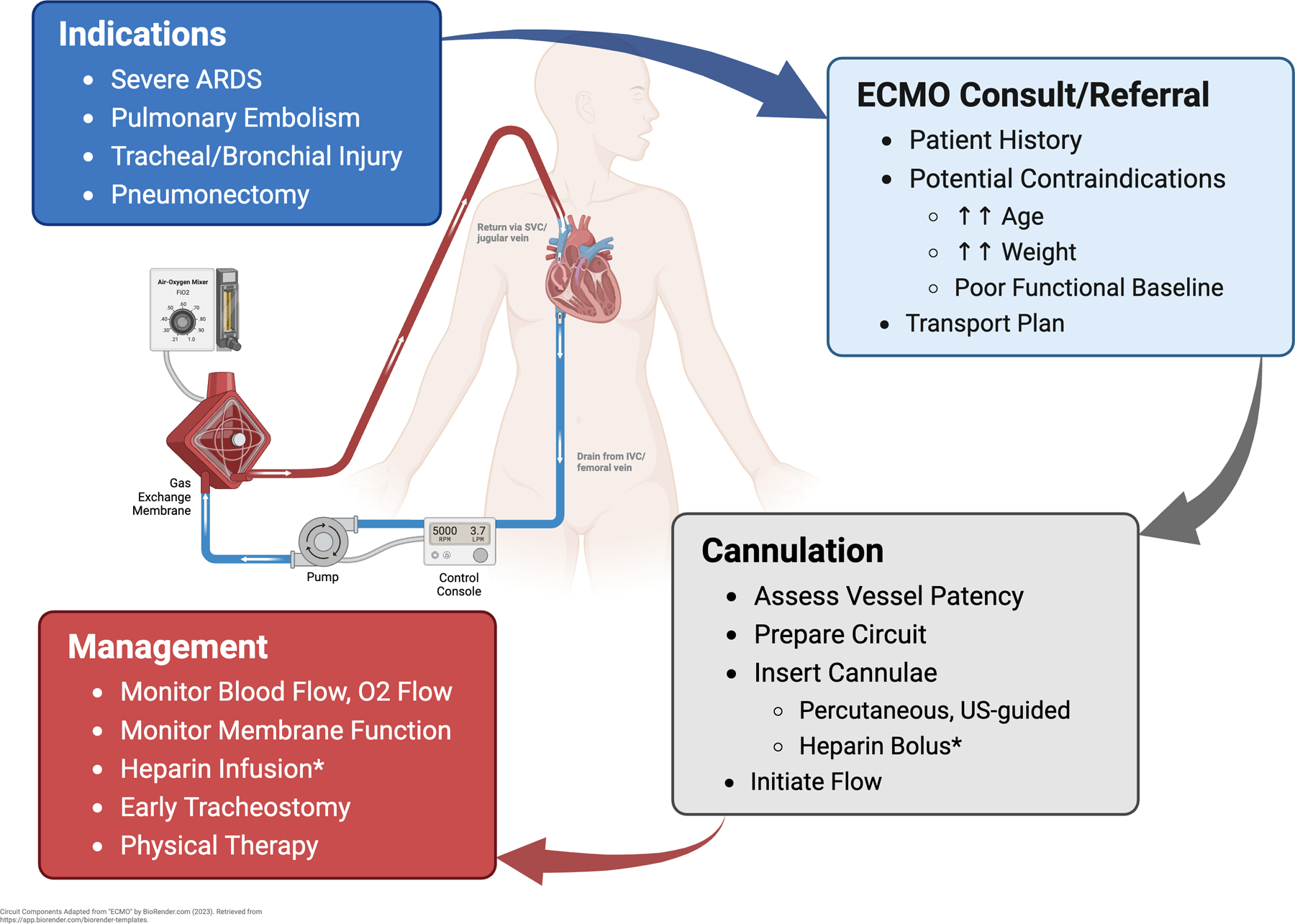
Over the past 10 years, extracorporeal membrane oxygenation (ECMO) use in trauma patients has increased significantly. This includes adult and pediatric trauma patients and even combat casualties. Most ECMO applications are in a venovenous (VV ECMO) configuration for acute hypoxemic respiratory failure or anatomic injuries that require pneumonectomy or extreme lung rest in a patient with insufficient respiratory reserve. In this narrative review, we summarize the most common indications for VV ECMO and other forms of ECMO support used in critically injured patients, underscore the importance of early ECMO consultation or regional referral, review the technical aspects of ECMO cannulation and management, and examine the expected outcomes for these patients. In addition, we evaluate the data where it exists to try to debunk some common myths surrounding ECMO management.
Copyright © 2023 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Figures



Similar articles
-
Extracorporeal membrane oxygenation for critically ill adults.Cochrane Database Syst Rev. 2015 Jan 22;1(1):CD010381. doi: 10.1002/14651858.CD010381.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2023 Sep 26;9:CD010381. doi: 10.1002/14651858.CD010381.pub3. PMID: 25608845 Free PMC article. Updated.
-
Extracorporeal membrane oxygenation for adult respiratory distress syndrome in trauma patients: A case series and systematic literature review.J Trauma Acute Care Surg. 2017 Jan;82(1):165-173. doi: 10.1097/TA.0000000000001276. J Trauma Acute Care Surg. 2017. PMID: 27779577
-
Anticoagulation Practices during Venovenous Extracorporeal Membrane Oxygenation for Respiratory Failure. A Systematic Review.Ann Am Thorac Soc. 2016 Dec;13(12):2242-2250. doi: 10.1513/AnnalsATS.201605-364SR. Ann Am Thorac Soc. 2016. PMID: 27690525
-
Safety and feasibility of conversion from venoarterial to venovenous extracorporeal membrane oxygenation in pediatric patients: A case series.Perfusion. 2025 Jul;40(5):1145-1150. doi: 10.1177/02676591241282578. Epub 2024 Sep 6. Perfusion. 2025. PMID: 39241122
-
Hemoadsorption in acute respiratory distress syndrome patients requiring venovenous extracorporeal membrane oxygenation: a systematic review.Respir Res. 2024 Jan 12;25(1):27. doi: 10.1186/s12931-024-02675-8. Respir Res. 2024. PMID: 38217010 Free PMC article.
Cited by
-
Current role of extracorporeal membrane oxygenation for the management of trauma patients: Indications and results.World J Crit Care Med. 2025 Mar 9;14(1):96694. doi: 10.5492/wjccm.v14.i1.96694. eCollection 2025 Mar 9. World J Crit Care Med. 2025. PMID: 40060741 Free PMC article. Review.
References
-
- Fortenberry JD, Lorusso, Roberto. Chapter 1: The History and Development of Extracorporeal Support. In: Brogan TVL, Laurance Lorusso, Roberto MacLaren, Graeme Peek, Giles, editor. Extracorporeal Life Support: The ELSO Red Book 5th Edition. Ann Arbor, Michigan: Extracorporeal Life Support Organization; 2017.
-
- Bartlett RH, Conrad Steven A. Chapter 4: The Physiology of Extracorporeal Life Support. In: Brogan TVL, Laurance Lorusso, Roberto MacLaren, Graeme Peek, Giles, editor. Extracorporeal Life Support: The ELSO Red Book 5th Edition. Ann Arbor, Michigan: Extracorporeal Life Support Organization; 2017.
-
- Miranda DR, Van Thiel R, Brodie D, Bakker J. Right ventricular unloading after initiation of venovenous extracorporeal membrane oxygenation. American Journal of Respiratory and Critical Care Medicine. 2015;191(3):346–8. - PubMed
-
- Tonna JE, Abrams D, Brodie D, Greenwood JC, Mateo-Sidron JAR, Usman A, et al. Management of adult patients supported with venovenous extracorporeal membrane oxygenation (VV ECMO): guideline from the extracorporeal life support organization (ELSO). ASAIO Journal (American Society for Artificial Internal Organs: 1992). 2021;67(6):601. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
