

A case of internal hernia in the pararectal fossa
- PMID: 37843687
- PMCID: PMC10579196
- DOI: 10.1186/s40792-023-01746-0
A case of internal hernia in the pararectal fossa
Abstract
Background: Internal hernias are relatively rare and difficult to diagnose. Diagnostic delays lead to the progression of strangulation. In particular, pararectal fossa hernias are extremely rare. We encountered a case in which internal hernia occurred in the pararectal fossa.
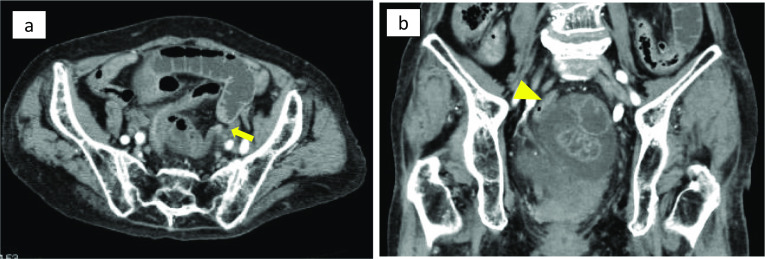
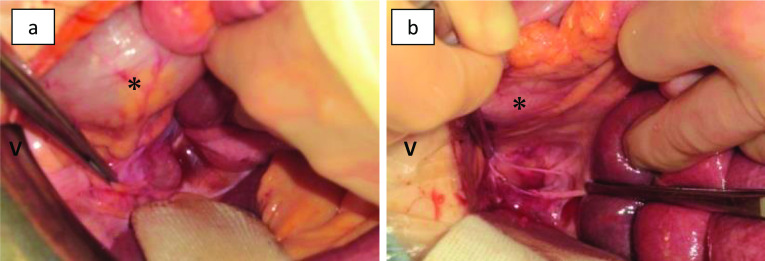
Case presentation: An 87-year-old woman was referred to our hospital because of persistent lower abdominal pain and vomiting. Contrast-enhanced computed tomography revealed findings of intestinal ischemia, such as closed loop formation with reduced contrast effect on the left side of the rectum in the pelvis. Strangulation small bowel obstruction was diagnosed, and emergency laparotomy was performed. The small intestine was found to invade the peritoneal reflection on the left side of the rectum. The patient was finally diagnosed with pararectal fossa hernia. The incarcerated small intestine was released with no bowel resection. The 4-cm hernia phylum was observed and closed by simple suture. The patient had a good postoperative course without recurrence.
Conclusions: We encountered a very rare case of internal hernia in the left pararectal fossa. Preoperative diagnosis of this disease is difficult, but it should nevertheless be considered in cases in which the cause of the intestinal obstruction is unknown.
Keywords: Internal hernia; Intestinal obstruction; Pararectal fossa hernia; Perirectal fossa hernia.
© 2023. Japan Surgical Society.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Steinke CR. Internal hernia: three additional case reports. Arch Surg. 1932;25(5):909–925. doi: 10.1001/archsurg.1932.01160230092008. - DOI
LinkOut - more resources
Full Text Sources
