

Etiology of White Matter Hyperintensities in Autosomal Dominant and Sporadic Alzheimer Disease
- PMID: 37843849
- PMCID: PMC10580156
- DOI: 10.1001/jamaneurol.2023.3618
Etiology of White Matter Hyperintensities in Autosomal Dominant and Sporadic Alzheimer Disease
Abstract
Importance: Increased white matter hyperintensity (WMH) volume is a common magnetic resonance imaging (MRI) finding in both autosomal dominant Alzheimer disease (ADAD) and late-onset Alzheimer disease (LOAD), but it remains unclear whether increased WMH along the AD continuum is reflective of AD-intrinsic processes or secondary to elevated systemic vascular risk factors.
Objective: To estimate the associations of neurodegeneration and parenchymal and vessel amyloidosis with WMH accumulation and investigate whether systemic vascular risk is associated with WMH beyond these AD-intrinsic processes.
Design, setting, and participants: This cohort study used data from 3 longitudinal cohort studies conducted in tertiary and community-based medical centers-the Dominantly Inherited Alzheimer Network (DIAN; February 2010 to March 2020), the Alzheimer's Disease Neuroimaging Initiative (ADNI; July 2007 to September 2021), and the Harvard Aging Brain Study (HABS; September 2010 to December 2019).
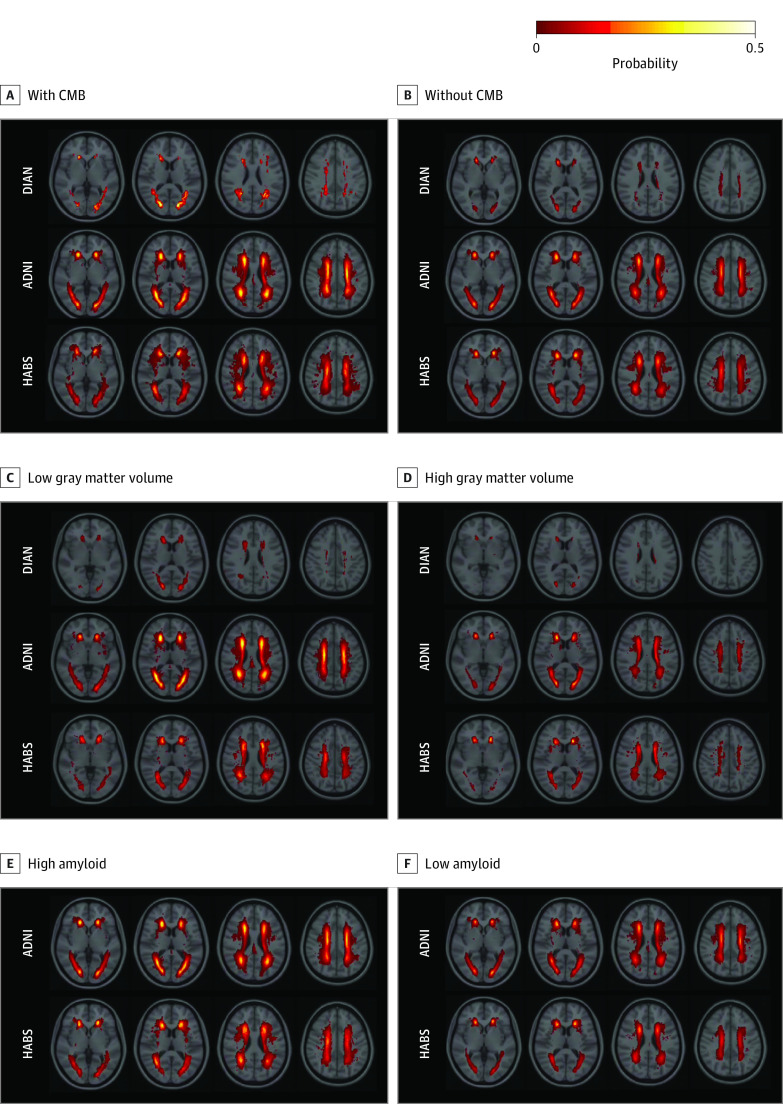
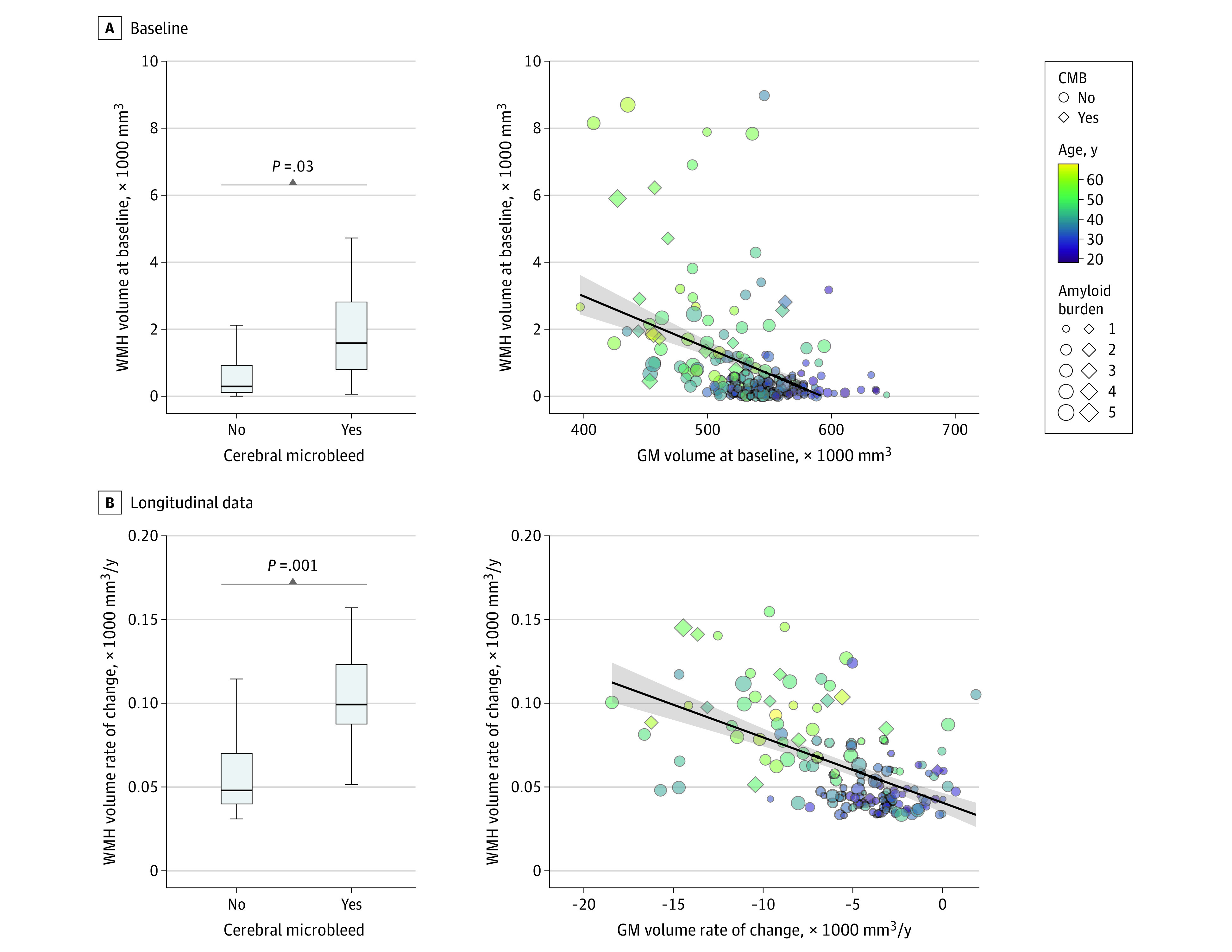
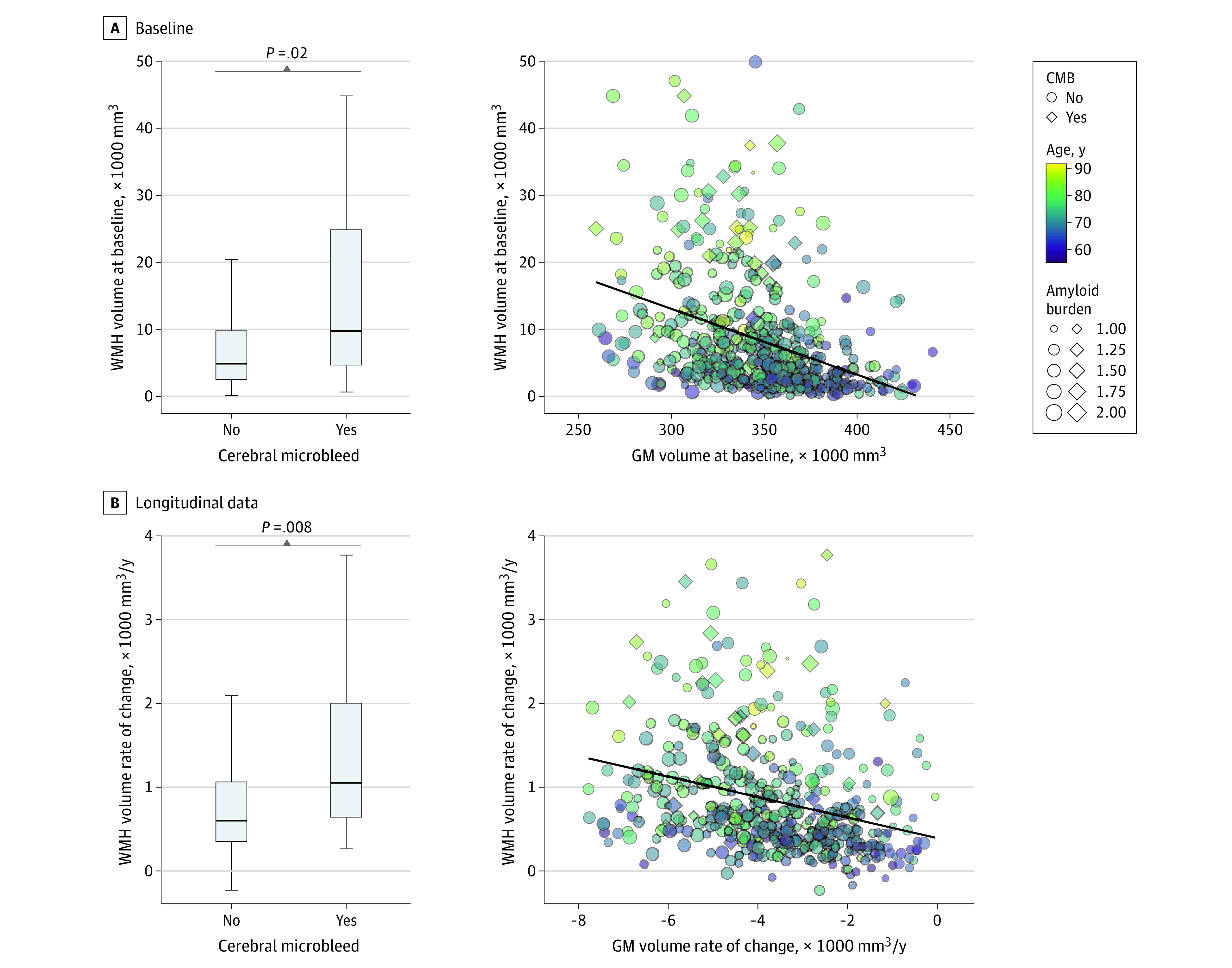
Main outcome and measures: The main outcomes were the independent associations of neurodegeneration (decreases in gray matter volume), parenchymal amyloidosis (assessed by amyloid positron emission tomography), and vessel amyloidosis (evidenced by cerebral microbleeds [CMBs]) with cross-sectional and longitudinal WMH.
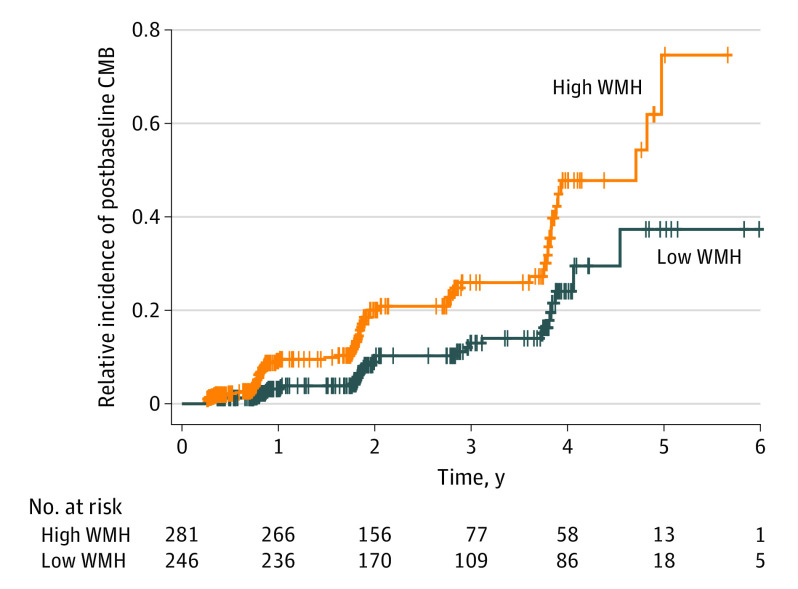
Results: Data from 3960 MRI sessions among 1141 participants were included: 252 pathogenic variant carriers from DIAN (mean [SD] age, 38.4 [11.2] years; 137 [54%] female), 571 older adults from ADNI (mean [SD] age, 72.8 [7.3] years; 274 [48%] female), and 318 older adults from HABS (mean [SD] age, 72.4 [7.6] years; 194 [61%] female). Longitudinal increases in WMH volume were greater in individuals with CMBs compared with those without (DIAN: t = 3.2 [P = .001]; ADNI: t = 2.7 [P = .008]), associated with longitudinal decreases in gray matter volume (DIAN: t = -3.1 [P = .002]; ADNI: t = -5.6 [P < .001]; HABS: t = -2.2 [P = .03]), greater in older individuals (DIAN: t = 6.8 [P < .001]; ADNI: t = 9.1 [P < .001]; HABS: t = 5.4 [P < .001]), and not associated with systemic vascular risk (DIAN: t = 0.7 [P = .40]; ADNI: t = 0.6 [P = .50]; HABS: t = 1.8 [P = .06]) in individuals with ADAD and LOAD after accounting for age, gray matter volume, CMB presence, and amyloid burden. In older adults without CMBs at baseline, greater WMH volume was associated with CMB development during longitudinal follow-up (Cox proportional hazards regression model hazard ratio, 2.63; 95% CI, 1.72-4.03; P < .001).
Conclusions and relevance: The findings suggest that increased WMH volume in AD is associated with neurodegeneration and parenchymal and vessel amyloidosis but not with elevated systemic vascular risk. Additionally, increased WMH volume may represent an early sign of vessel amyloidosis preceding the emergence of CMBs.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- P30 AG066444/AG/NIA NIH HHS/United States
- P30 AG066512/AG/NIA NIH HHS/United States
- P01 AG036694/AG/NIA NIH HHS/United States
- P01 AG003991/AG/NIA NIH HHS/United States
- K01 AG080123/AG/NIA NIH HHS/United States
- P30 AG066530/AG/NIA NIH HHS/United States
- UF1 AG032438/AG/NIA NIH HHS/United States
- P30 AG072947/AG/NIA NIH HHS/United States
- P30 AG072972/AG/NIA NIH HHS/United States
- P30 AG066514/AG/NIA NIH HHS/United States
- P01 AG026276/AG/NIA NIH HHS/United States
- U01 AG024904/AG/NIA NIH HHS/United States
- S10 RR023401/RR/NCRR NIH HHS/United States
- RF1 AG079569/AG/NIA NIH HHS/United States
- P30 AG072977/AG/NIA NIH HHS/United States
- P41 EB015896/EB/NIBIB NIH HHS/United States
- S10 RR023043/RR/NCRR NIH HHS/United States
- U19 AG032438/AG/NIA NIH HHS/United States
- R01 NS092865/NS/NINDS NIH HHS/United States
- S10 RR021110/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
