

Optimising prediction of mortality, stroke, and major bleeding for patients with atrial fibrillation: validation of the GARFIELD-AF tool in UK primary care electronic records
- PMID: 37845083
- PMCID: PMC10587901
- DOI: 10.3399/BJGP.2023.0082
Optimising prediction of mortality, stroke, and major bleeding for patients with atrial fibrillation: validation of the GARFIELD-AF tool in UK primary care electronic records
Abstract
Background: The GARFIELD-AF tool is a novel risk tool that simultaneously assesses the risk of all-cause mortality, stroke or systemic embolism, and major bleeding in patients with atrial fibrillation (AF).
Aim: To validate the GARFIELD-AF tool using UK primary care electronic records.
Design and setting: A retrospective cohort study using the Clinical Practice Research Datalink (CPRD) linked with Hospital Episode Statistics data and Office for National Statistics mortality data.
Method: Discrimination was evaluated using the area under the curve (AUC) and calibration was evaluated using calibration-in-the-large regression and calibration plots.
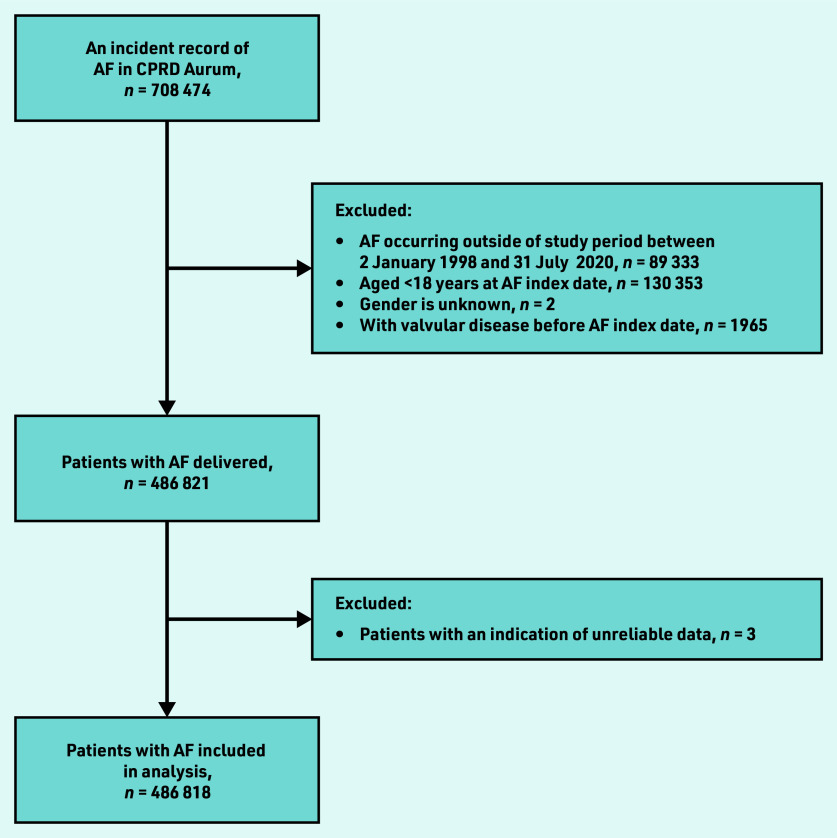
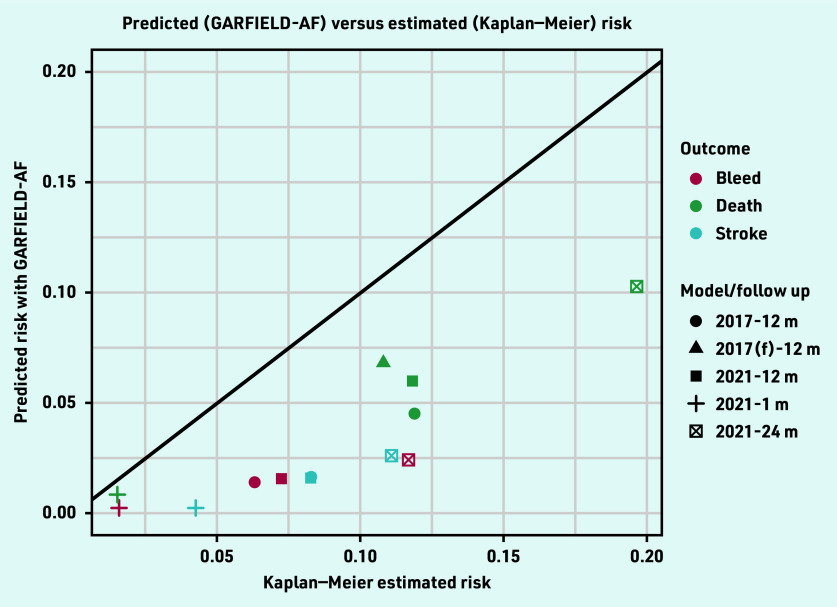
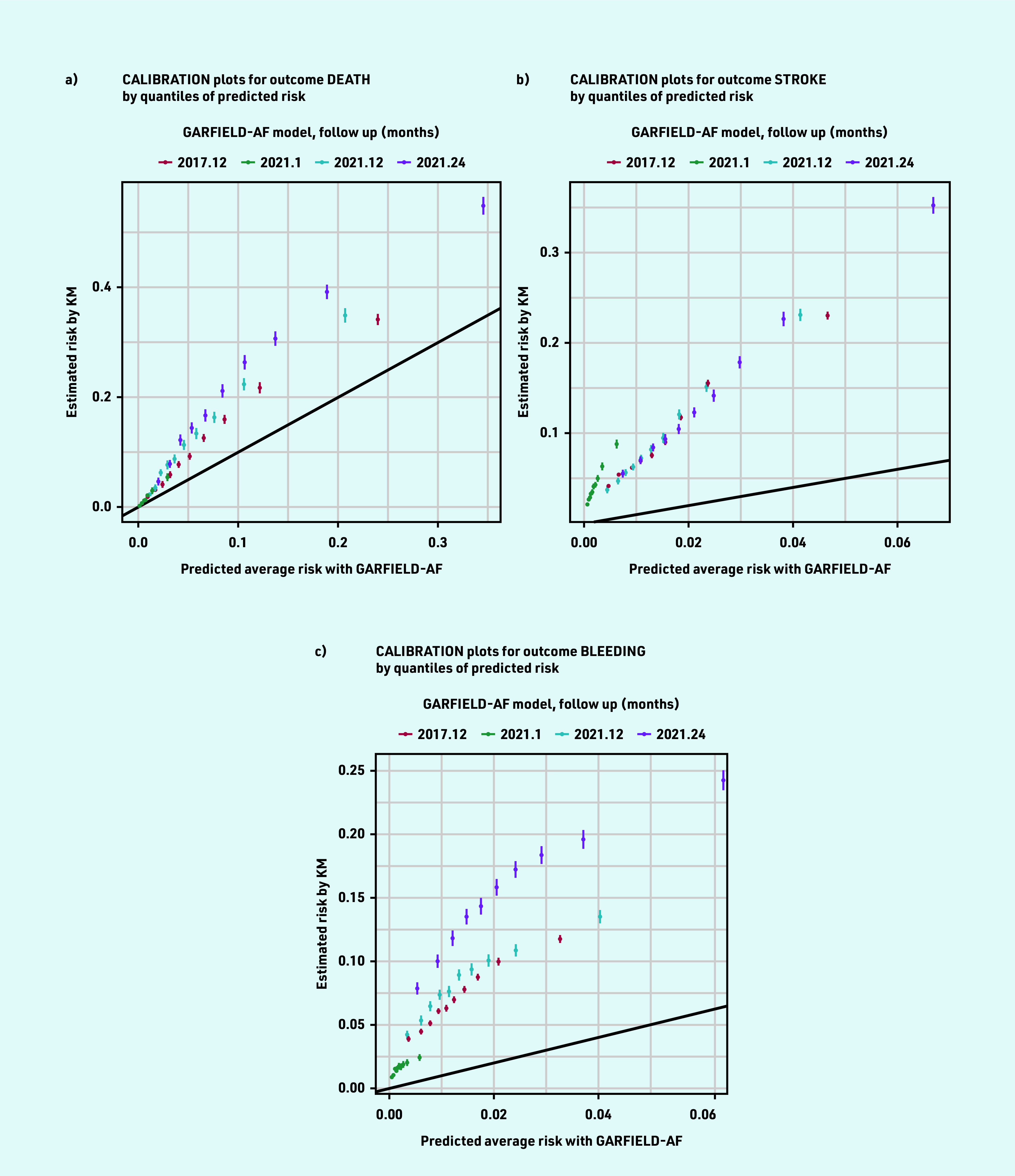
Results: A total of 486 818 patients aged ≥18 years with incident diagnosis of non-valvular AF between 2 January 1998 and 31 July 2020 were included; 50.6% (n = 246 425/486 818) received anticoagulation at diagnosis The GARFIELD- AF models outperformed the CHA2DS2VASc and HAS-BLED scores in discrimination ability of death, stroke, and major bleeding at all the time points. The AUC for events at 1 year for the 2017 models were: death 0.747 (95% confidence interval [CI] = 0.744 to 0.751) versus 0.635 (95% CI = 0.631 to 0.639) for CHA2DS2VASc; stroke 0.666 (95% CI = 0.663 to 0.669) versus 0.625 (95% CI = 0.622 to 0.628) for CHA2DS2VASc; and major bleeding 0.602 (95% CI = 0.598 to 0.606) versus 0.558 (95% CI = 0.554 to 0.562) for HAS- BLED. Calibration between predicted and Kaplan- Meier observed events was inadequate with the GARFIELD-AF models.
Conclusion: The GARFIELD-AF models were superior to the CHA2DS2VASc score for discriminating stroke and death and superior to the HAS-BLED score for discriminating major bleeding. The models consistently underpredicted the level of risk, suggesting that a recalibration is needed to optimise its use in the UK population.
Keywords: all-cause mortality; anticoagulation; atrial fibrillation; bleeding; risk stratification; stroke.
© The Authors.
Conflict of interest statement
The authors have declared no competing interests.
Figures
References
-
- Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation: analysis of pooted data from five randomized controlled trials. Arch Intern Med. 1994;154(13):1449–1457. - PubMed
-
- Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–498. - PubMed
-
- National Institute for Health and Care Excellence Atrial fibrillation: diagnosis and management. NG196. 2021 https://www.nice.org.uk/guidance/ng196 (accessed 5 Oct 2023). - PubMed
-
- NHS Digital Quality and Outcomes Framework, achievement, prevalence and exceptions data 2018–19 [PAS] 2019. https://digital.nhs.uk/data-and-information/publications/statistical/qua... (accessed 5 Oct 2023).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical