

Bifidobacteria metabolize lactulose to optimize gut metabolites and prevent systemic infection in patients with liver disease
- PMID: 37845315
- PMCID: PMC11059310
- DOI: 10.1038/s41564-023-01493-w
Bifidobacteria metabolize lactulose to optimize gut metabolites and prevent systemic infection in patients with liver disease
Abstract
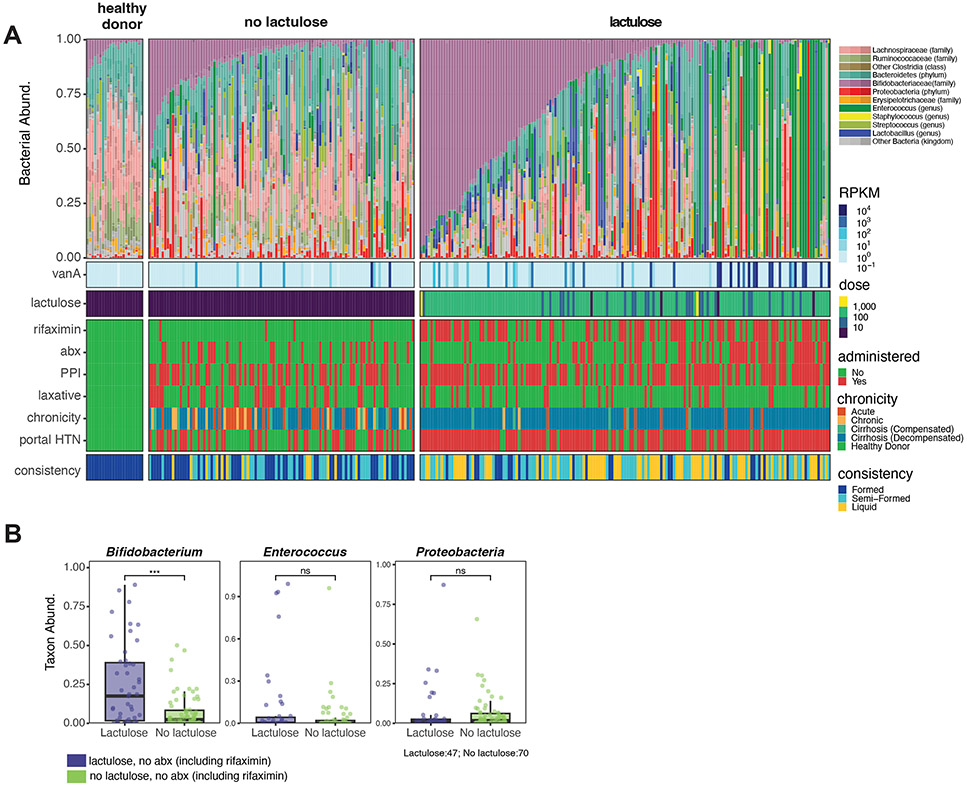
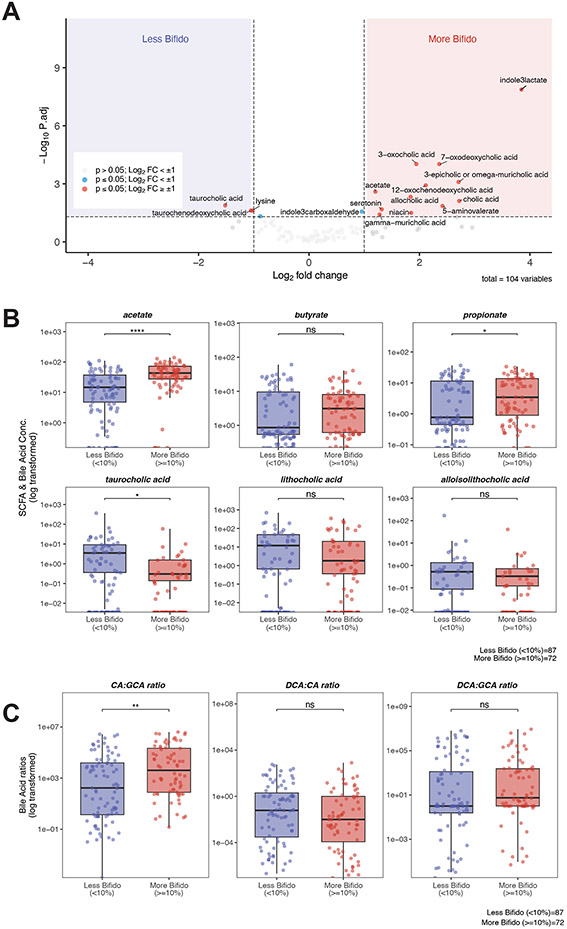
Progression of chronic liver disease is precipitated by hepatocyte loss, inflammation and fibrosis. This process results in the loss of critical hepatic functions, increasing morbidity and the risk of infection. Medical interventions that treat complications of hepatic failure, including antibiotic administration for systemic infections and lactulose treatment for hepatic encephalopathy, can impact gut microbiome composition and metabolite production. Here, using shotgun metagenomic sequencing and targeted metabolomic analyses on 847 faecal samples from 262 patients with acute or chronic liver disease, we demonstrate that patients hospitalized for liver disease have reduced microbiome diversity and a paucity of bioactive metabolites, including short-chain fatty acids and bile acid derivatives, that impact immune defences and epithelial barrier integrity. We find that patients treated with the orally administered but non-absorbable disaccharide lactulose have increased densities of intestinal bifidobacteria and reduced incidence of systemic infections and mortality. Bifidobacteria metabolize lactulose, produce high concentrations of acetate and acidify the gut lumen in humans and mice, which, in combination, can reduce the growth of antibiotic-resistant bacteria such as vancomycin-resistant Enterococcus faecium in vitro. Our studies suggest that lactulose and bifidobacteria serve as a synbiotic to reduce rates of infection in patients with severe liver disease.
© 2023. The Author(s), under exclusive licence to Springer Nature Limited.
Figures



Comment in
-
Pleiotropic prebiotic for liver disease.Nat Microbiol. 2023 Nov;8(11):1944-1945. doi: 10.1038/s41564-023-01510-y. Nat Microbiol. 2023. PMID: 37845317 No abstract available.
-
Deploying Lactulose as a Prebiotic to Reduce Complications of Chronic Liver Disease.Gastroenterology. 2024 Mar;166(3):534-535. doi: 10.1053/j.gastro.2023.11.287. Epub 2023 Nov 23. Gastroenterology. 2024. PMID: 38000683 No abstract available.
References
-
- Younossi ZM et al. Epidemiology of chronic liver diseases in the USA in the past three decades. Gut 69, 564 (2020). - PubMed
-
- Franchis R. de et al. BAVENO VII - RENEWING CONSENSUS IN PORTAL HYPERTENSION Report of the Baveno VII Consensus Workshop: personalized care in portal hypertension. J Hepatol 76, 959–974 (2021). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
