

Adjuvant nivolumab in resected stage IIB/C melanoma: primary results from the randomized, phase 3 CheckMate 76K trial
- PMID: 37845511
- PMCID: PMC10667090
- DOI: 10.1038/s41591-023-02583-2
Adjuvant nivolumab in resected stage IIB/C melanoma: primary results from the randomized, phase 3 CheckMate 76K trial
Erratum in
-
Publisher Correction: Adjuvant nivolumab in resected stage IIB/C melanoma: primary results from the randomized, phase 3 CheckMate 76K trial.Nat Med. 2024 Feb;30(2):607. doi: 10.1038/s41591-023-02661-5. Nat Med. 2024. PMID: 37923838 Free PMC article. No abstract available.
-
Author Correction: Adjuvant nivolumab in resected stage IIB/C melanoma: primary results from the randomized, phase 3 CheckMate 76K trial.Nat Med. 2024 Mar;30(3):906. doi: 10.1038/s41591-023-02775-w. Nat Med. 2024. PMID: 38177857 Free PMC article. No abstract available.
Abstract
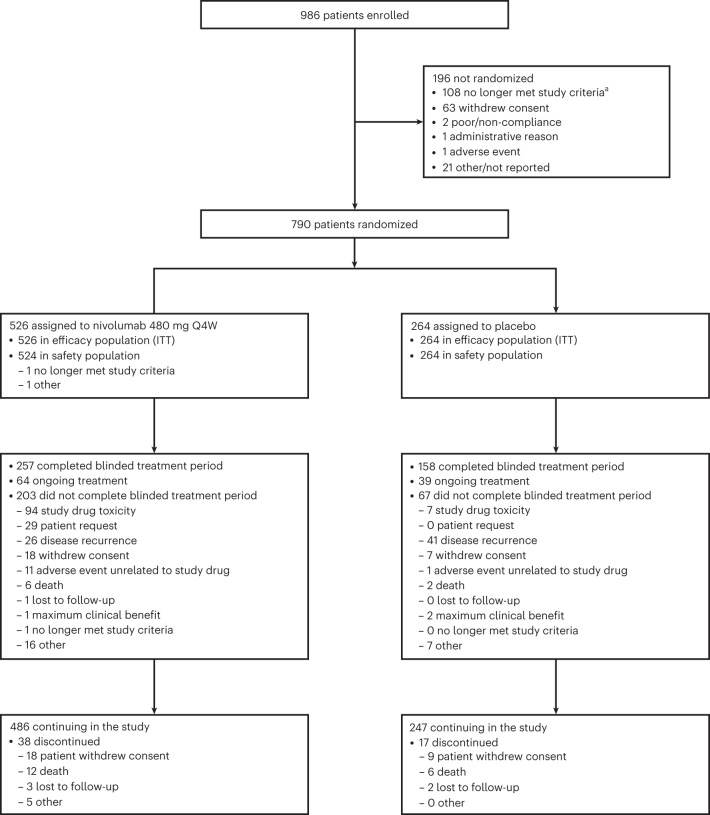
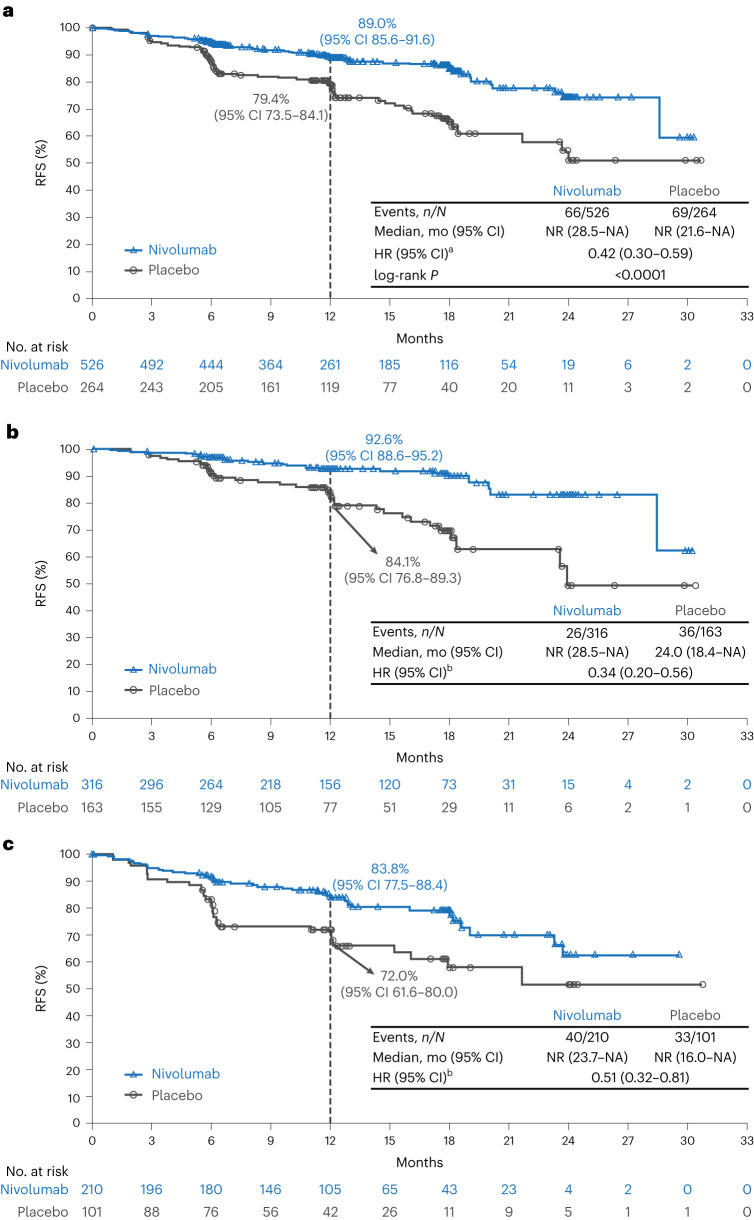
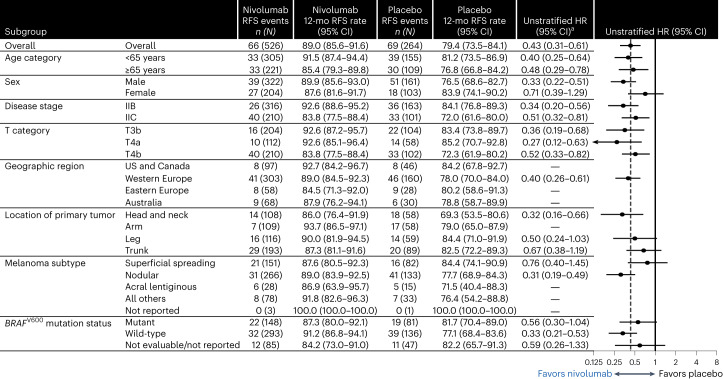
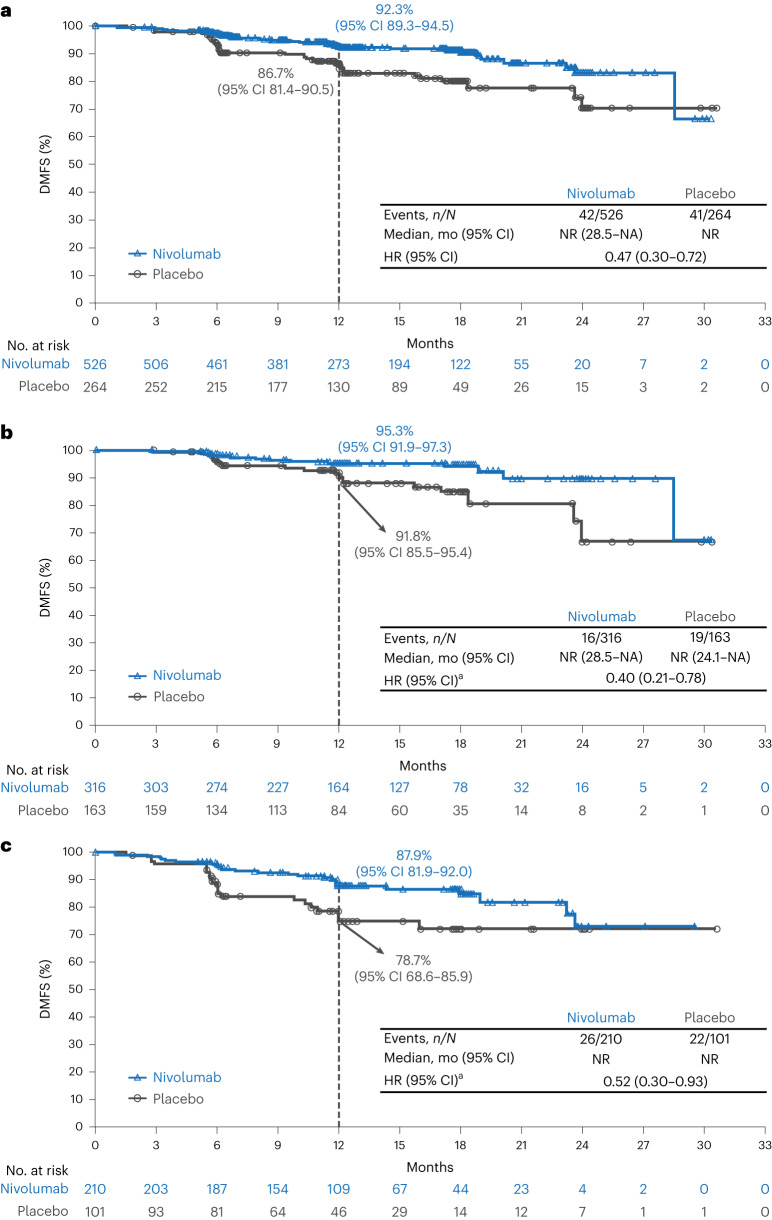
Patients with resected stage IIB/C melanoma have high recurrence risk, similar to those with resected stage IIIA/B disease. The phase 3, double-blind CheckMate 76K trial assessed 790 patients with resected stage IIB/C melanoma randomized 2:1 (stratified by tumor category) to nivolumab 480 mg or placebo every 4 weeks for 12 months. The primary endpoint was investigator-assessed recurrence-free survival (RFS). Secondary endpoints included distant metastasis-free survival (DMFS) and safety. At 7.8 months of minimum follow-up, nivolumab significantly improved RFS versus placebo (hazard ratio (HR) = 0.42; 95% confidence interval (CI): 0.30-0.59; P < 0.0001), with 12-month RFS of 89.0% versus 79.4% and benefit observed across subgroups; DMFS was also improved (HR = 0.47; 95% CI: 0.30-0.72). Treatment-related grade 3/4 adverse events occurred in 10.3% (nivolumab) and 2.3% (placebo) of patients. One treatment-related death (0.2%) occurred with nivolumab. Nivolumab is an effective and generally well-tolerated adjuvant treatment in patients with resected stage IIB/C melanoma. ClinicalTrials.gov identifier: NCT04099251 .
© 2023. The Author(s).
Conflict of interest statement
J.M.K. reports research funding received by his institution from Amgen, Bristol Myers Squibb, Checkmate Pharmaceuticals, Harbour BioMed, Immvira Pharma Co., Immunocore, Iovance Biotherapeutics, Lion Biotechnologies, Novartis, Takeda and Verastem; consulting fees from Amgen, Ankyra Therapeutics, Applied Clinical Intelligence, Becker Pharmaceutical Consulting, Bristol Myers Squibb, Cancer Network, Cancer Study Group, Checkmate Pharmaceuticals, DermTech, Fenix Group International, Harbour BioMed, Immunocore, iOnctura, Iovance Biotherapeutics, Istari Oncology, Jazz Pharmaceuticals, Magnolia Innovation, Merck, Natera, Novartis, OncoCyte Corporation, OncoSec Medical, PathAI, Pfizer, Regeneron, Replimune, Scopus BioPharma, SR One Capital Management, LP and Takeda; honoraria from Bristol Myers Squibb; meeting/travel support from Ankyra Therapeutics, Checkmate Pharmaceuticals, Iovance Biotherapeutics and Regeneron; participation on data safety monitoring/advisory boards for Axio Research and IQVIA; and leadership positions at AIM at Melanoma. M.D.V. reports consulting fees from Bristol Myers Squibb, Immunocore, Merck Sharp & Dohme, Novartis and Pierre Fabre; honoraria from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis and Pierre Fabre; and meeting/travel support from Pierre Fabre. J.W. reports research funding received by his institution from Bristol Myers Squibb; consulting fees from AstraZeneca, Bristol Myers Squibb, Genentech, Incyte, Merck, Pfizer and Regeneron; honoraria from Bristol Myers Squibb; meeting/travel support from Bristol Myers Squibb; being named on a patent for a PD-1 inhibitor developed by Biodesix unrelated to this study; and being a shareholder of Biond, Evaxion, Instil Bio and OncoC4. C.H. reports research funding received by his institution from Amgen, BioNTech, Bristol Myers Squibb, Merck Sharp & Dohme, Nektar, Novartis, Pierre Fabre and Regeneron; consulting fees from Almirall, Amgen, Bristol Myers Squibb, Immunocore, Merck Sharp & Dohme, Novartis, Pierre Fabre, Roche and Sanofi; honoraria from Amgen, Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Roche and Sanofi; meeting/travel support from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis and Pierre Fabre; participation on data safety monitoring/advisory boards for Amgen; and leadership positions at the Austrian Society of Dermatology and Venerology, the European Association of Dermato-Oncology and the European Society for Medical Oncology Melanoma Group. J.-J.G. reports research funding received by his institution from Pierre Fabre; consulting fees from Amgen, Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Philogen, Pierre Fabre and Sanofi; honoraria from Bristol Myers Squibb, Novartis and Pierre Fabre; meeting/travel support from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis and Pierre Fabre; and participation on data safety monitoring/advisory boards for Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Philogen, Pierre Fabre and Sanofi. P.M. reports research funding received by his institution from Bristol Myers Squibb, Merck Sharp & Dohme and Novartis; consulting fees from Almirall Hermal, Amgen, Beiersdorf, Bristol Myers Squibb, Immunocore, Merck, Merck Sharp & Dohme, Novartis, Pfizer, Pierre Fabre, Regeneron, Sanofi and Sun Pharma; honoraria from Amgen, Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre Fabre, Sanofi and Sun Pharma; meeting/travel support from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre Fabre and Sun Pharma; and leadership positions at Melanom Info Deutschland. C.L. reports consulting fees from Almirall Hermal, BioNTech, Bristol Myers Squibb, Immunocore, Kyowa Kirin, Merck, Merck Sharp & Dohme, Novartis, Pierre Fabre, Roche, Sanofi and Sun Pharma; honoraria from Almirall Hermal, BioNTech, Bristol Myers Squibb, Immunocore, Kyowa Kirin, Merck, Merck Sharp & Dohme, Novartis, Pierre Fabre, Roche, Sanofi and Sun Pharma; meeting/travel support from Almirall Hermal, BioNTech, Bristol Myers Squibb, Immunocore, Kyowa Kirin, Merck, Merck Sharp & Dohme, Novartis, Pierre Fabre, Roche, Sanofi and Sun Pharma; and participation on data safety monitoring/advisory boards for Almirall Hermal, BioNTech, Bristol Myers Squibb, Immunocore, Kyowa Kirin, Merck, Merck Sharp & Dohme, Novartis, Pierre Fabre, Roche, Sanofi and Sun Pharma. C.D. reports consulting fees from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre Fabre, Sanofi and Sun Pharma; honoraria from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre Fabre, Sanofi and Sun Pharma; and meeting/travel support from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre Fabre, Sanofi and Sun Pharma. V.S.-C. reports meeting/travel support from Pierre Fabre and Sun Pharma and participation on advisory boards for Merck Sharp & Dohme and Pierre Fabre. J.M. reports honoraria from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre Fabre and Roche; meeting/travel support from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Pierre Fabre and Roche; and participation on data safety monitoring/advisory boards for Bristol Myers Squibb, Merck Sharp & Dohme and Novartis. P.R. reports consulting fees from Blueprint Medicines, Bristol Myers Squibb, Merck, Merck Sharp & Dohme, Novartis, Philogen, Pierre Fabre and Sanofi and honoraria from AstraZeneca, Blueprint Medicines, Bristol Myers Squibb, Merck, Merck Sharp & Dohme, Novartis, Philogen, Pierre Fabre and Sanofi. T.M.M. reports research funding received by his institution from Bristol Myers Squibb; consulting fees from AstraZeneca, Bristol Myers Squibb, Eisai, GlaxoSmithKline, Merck, Merck Sharp & Dohme and Novartis; honoraria from AstraZeneca; meeting/travel support from AstraZeneca and Bristol Myers Squibb; and participation on data safety monitoring/advisory boards for AstraZeneca, Bristol Myers Squibb, Eisai, GlaxoSmithKline, Merck, Merck Sharp & Dohme and Novartis. P.A.A. reports research funding received by his institution from Array BioPharma, Bristol Myers Squibb, Genentech, Pfizer, Roche and Sanofi; consulting fees from 4SC, Array BioPharma, Bayer, Bio-Al Health, Bristol Myers Squibb, Genentech, Idera, Italfarmaco, Lunaphore, Medicenna, Merck Serono, Merck Sharp & Dohme, Nektar, Novartis, Pfizer, Pierre Fabre, Replimune, Roche, Sandoz, Sanofi, Sun Pharma and ValoTx; meeting/travel support from Bio-Al Health, Pfizer and Replimune; and participation on data safety monitoring/advisory boards for AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Eisai, Erasca, Genentech, Immunocore, iTeos, Merck Sharp & Dohme, Nouscom, Novartis, Oncosec, Regeneron, Roche and Seagen. A.M.M. reports consulting fees from Bristol Myers Squibb, Merck Sharp & Dohme, Novartis, Roche, Pierre Fabre and QBiotics. P.D. reports being an employee and shareholder of Bristol Myers Squibb. M.L. reports being an employee and shareholder of Bristol Myers Squibb. F.C. reports being an employee and shareholder of Bristol Myers Squibb. B.G. reports research funding received by his institution from Bristol Myers Squibb. G.V.L. reports consulting fees from Agenus, Amgen, Array BioPharma, Boehringer Ingelheim, Bristol Myers Squibb, Evaxion Biotech, Hexal AG, Highlight Therapeutics, Innovent Biologics USA, Merck Sharp & Dohme, Novartis, OncoSec Medical Australia, Pierre Fabre, Provectus Australia, QBiotics Group Limited and Regeneron; honoraria from Bristol Myers Squibb and Pierre Fabre; and participation on advisory boards for Agenus, Amgen, Array BioPharma, Boehringer Ingelheim, Bristol Myers Squibb, Evaxion Biotech, Hexal AG, Highlight Therapeutics, Innovent Biologics USA, Merck Sharp & Dohme, Novartis, OncoSec Medical Australia, Pierre Fabre, Provectus Australia, QBiotics Group Limited and Regeneron. All other authors have no competing interests to disclose.
Figures



References
-
- National Cancer Institute. The Surveillance, Epidemiology, and End Results (SEER) cancer stat facts: melanoma of the skin. https://seer.cancer.gov/statfacts/html/melan.html (2023).
-
- National Cancer Institute. The Surveillance, Epidemiology, and End Results (SEER)*Explorer: an interactive website for SEER cancer statistics. https://seer.cancer.gov/explorer (2023).
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
