

Resmetirom for nonalcoholic fatty liver disease: a randomized, double-blind, placebo-controlled phase 3 trial
- PMID: 37845512
- PMCID: PMC10667098
- DOI: 10.1038/s41591-023-02603-1
Resmetirom for nonalcoholic fatty liver disease: a randomized, double-blind, placebo-controlled phase 3 trial
Abstract
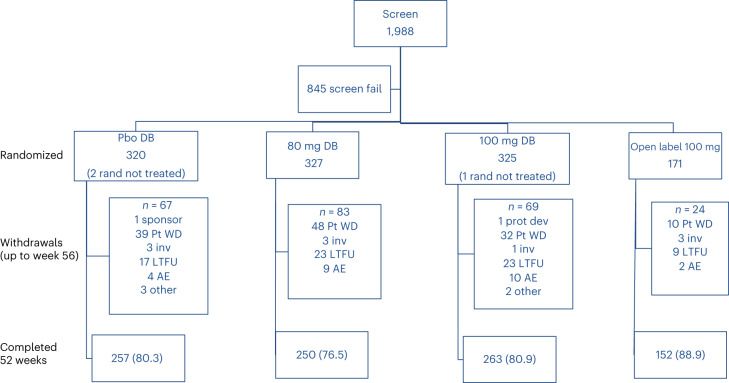
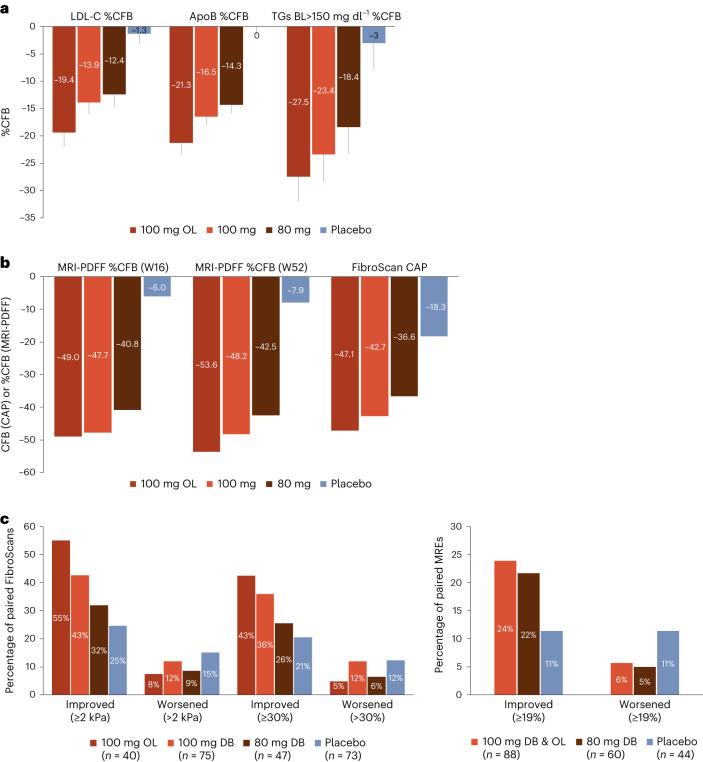
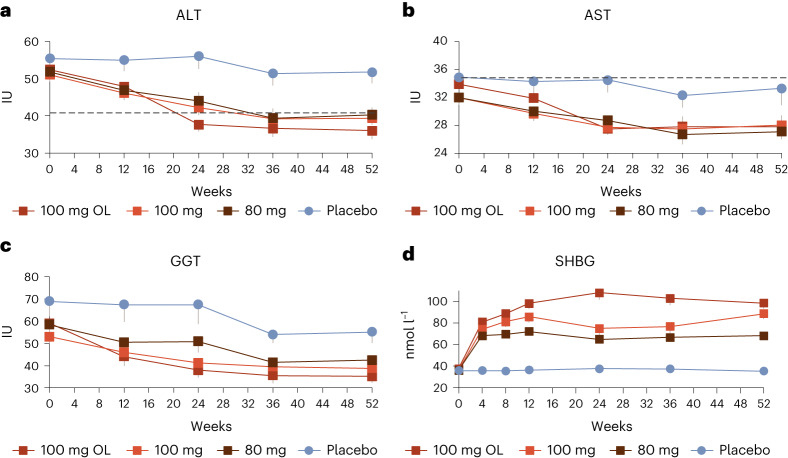
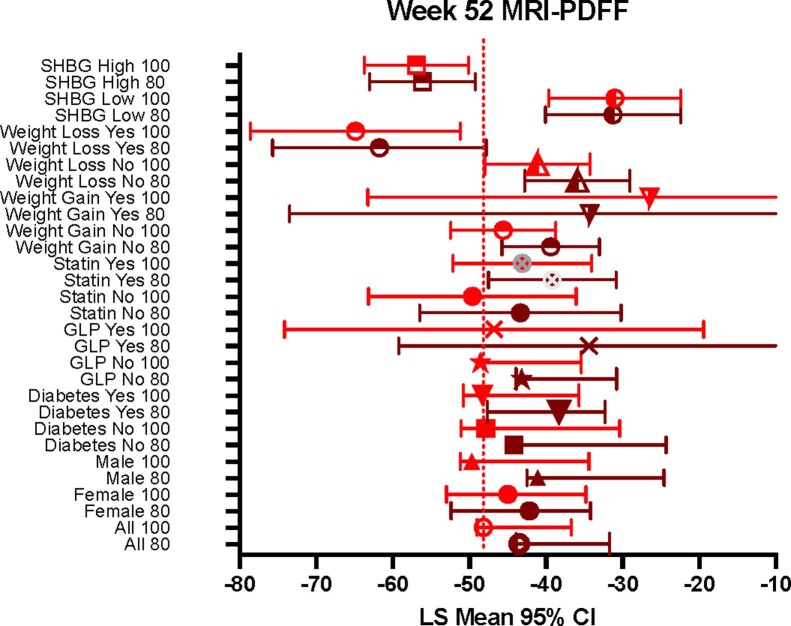
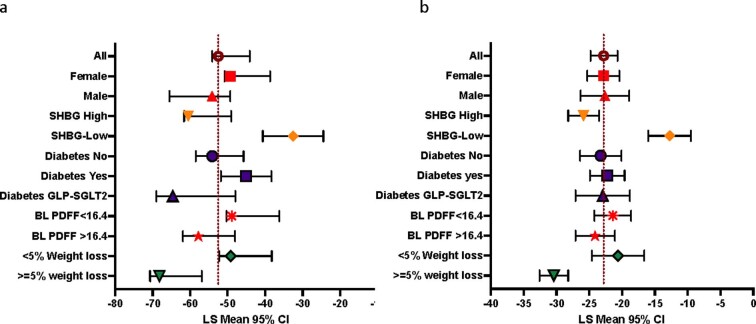
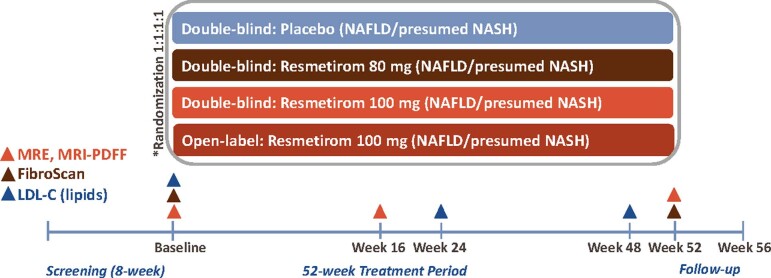
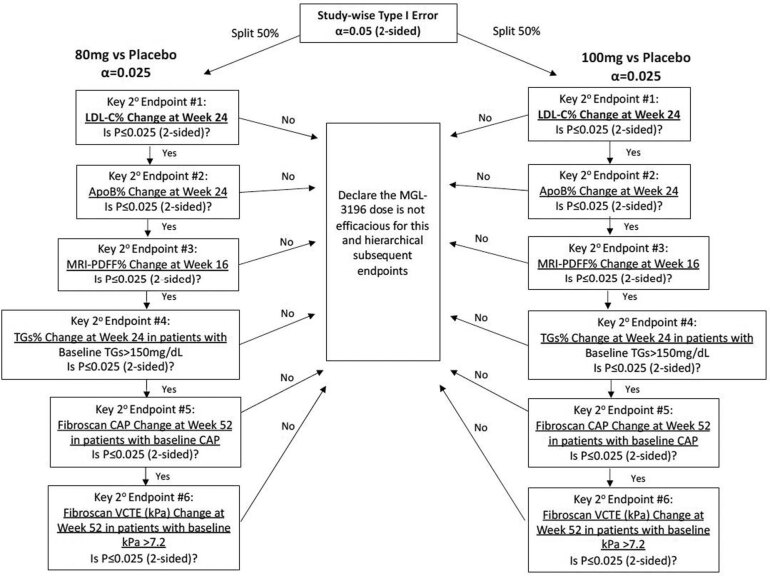
Nonalcoholic steatohepatitis (NASH) is a progressive liver disease with no approved treatment. MAESTRO-NAFLD-1 was a 52-week randomized, double-blind, placebo-controlled phase 3 trial evaluating the safety of resmetirom in adults with nonalcoholic fatty liver disease and presumed NASH. Patients were randomized to three double-blind arms (100 mg resmetirom (n = 325), 80 mg resmetirom (n = 327) or placebo (n = 320)) or open-label 100 mg resmetirom (n = 171). The primary end point was incidence of treatment-emergent adverse events (TEAEs) over 52 weeks and key secondary end points were LDL-C, apoB, triglycerides (over 24 weeks), hepatic fat (over 16 and 52 weeks) and liver stiffness (over 52 weeks). Resmetirom was safe and well tolerated. TEAEs occurred in 86.5% (open-label 100 mg resmetirom), 86.1% (100 mg resmetirom), 88.4% (80 mg resmetirom) and 81.8% (placebo) of patients. TEAEs in excess of placebo included diarrhea and nausea at the initiation of treatment. Key secondary end points included least square means difference from placebo at 80 mg, 100 mg resmetirom: LDL-C (-11.1%, -12.6%), apoB (-15.6%, -18.0%), triglycerides (-15.4%, -20.4%), 16-week hepatic fat (-34.9%, -38.6%), (P < 0.0001) and liver stiffness (-1.02, -1.70) and 52-week hepatic fat (-28.8, -33.9). These findings demonstrate resmetirom was safe and well tolerated in adults with presumed NASH, supporting a role for further clinical development. (ClinicalTrials.gov identifier NCT04197479 ).
© 2023. The Author(s).
Conflict of interest statement
S.A.H. reports grant/research support from 89 Bio, Boehringer Ingelheim, Akero, Altimmune, Axcella, Corcept, Cymabay, Enyo, Galectin, Galmed, Genentech, Genfit, Gilead, Hepion, Hightide, Intercept, Madrigal, Metacrine, NGM Bio, NorthSea, Poxel, Sagimet and Viking; advisory/consulting fees from Akero, Altimmune, AstraZeneca, Axcella, Chronic Liver Disease Foundation, Echosens, Genfit, Gilead, GSK, Hepion, Hepta Bio, Hightide, HistoIndex, Intercept, Madrigal, Medpace, NGM Bio, Northsea, Novartis, Novo Nordisk, Perspectum, Poxel, Sagimet, Sonic Incytes, Terns and Viking; and is the owner of Pinnacle Clinical Research. R.T. is an employee and stockholder at Madrigal Pharmaceuticals. G.W.N. reports advisory/consulting fees from Boehringer Ingelheim; grant/research support from Madrigal Pharmaceuticals; and speaker’s fees from Intercept Pharmaceuticals. K.J.L. reports grant/research support from Madrigal Pharmaceuticals. D.L. is an employee at Madrigal Pharmaceuticals. S.E.M. reports grant/research support from Madrigal Pharmaceuticals; owns stock in Madrigal Pharmaceuticals. N.A. reports grant/research support from 89Bio, AbbVie/Allergan, Akero, Better Therapeutics, Boehringer Ingelheim, Bristol-Myers Squibb, Corcept, DSM, Galectin, Genentech, Genfit, Gilead, Hepagene, Healio, Intercept, Inventiva, Ionis, Madrigal, Merck, NGM, Noom, NorthSea, Novo Nordisk, Perspectum, Pfizer, Poxel, Viking and Zydus; speaker’s fees from AbbVie/Allergan, Alexion, Echosens, Eisai, Exelixis, Gilead, Intercept, Perspectum, Salix and Theratechnologies; Consultant for AbbVie/Allergan, Echosens, Fibronostics, Gilead, Intercept, Madrigal, Novo Nordisk, Perspectum, Pfizer and Zydus. M.R.B. reports grant/research support from Carmot Therapeutics, Corcept Therapeutics, Madrigal Pharmaceuticals, Metacrine, NGM Biopharmaceuticals, Pinnacle Clinical Research, ProSciento and Siemens Healthineers; and advisory/consulting fees from Medpace.
Figures
Comment in
-
Resmetirom for metabolic dysfunction-associated steatohepatitis: targeting hepatic and cardiovascular disease.Hepatobiliary Surg Nutr. 2024 Dec 1;13(6):1034-1037. doi: 10.21037/hbsn-24-568. Epub 2024 Nov 14. Hepatobiliary Surg Nutr. 2024. PMID: 39669094 Free PMC article. No abstract available.
-
Resmetirom as an important cornerstone of multidisciplinary management of metabolic dysfunction-associated steatohepatitis.Hepatobiliary Surg Nutr. 2025 Apr 1;14(2):290-294. doi: 10.21037/hbsn-2024-716. Epub 2025 Mar 25. Hepatobiliary Surg Nutr. 2025. PMID: 40342776 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
