

Perinatal Azithromycin Provides Limited Neuroprotection in an Ovine Model of Neonatal Hypoxic-Ischemic Encephalopathy
- PMID: 37846563
- PMCID: PMC10589434
- DOI: 10.1161/STROKEAHA.123.043040
Perinatal Azithromycin Provides Limited Neuroprotection in an Ovine Model of Neonatal Hypoxic-Ischemic Encephalopathy
Abstract
Background: Hypoxic-ischemic brain injury/encephalopathy affects about 1.15 million neonates per year, 96% of whom are born in low- and middle-income countries. Therapeutic hypothermia is not effective in this setting, possibly because injury occurs significantly before birth. Here, we studied the pharmacokinetics, safety, and efficacy of perinatal azithromycin administration in near-term lambs following global ischemic injury to support earlier treatment approaches.
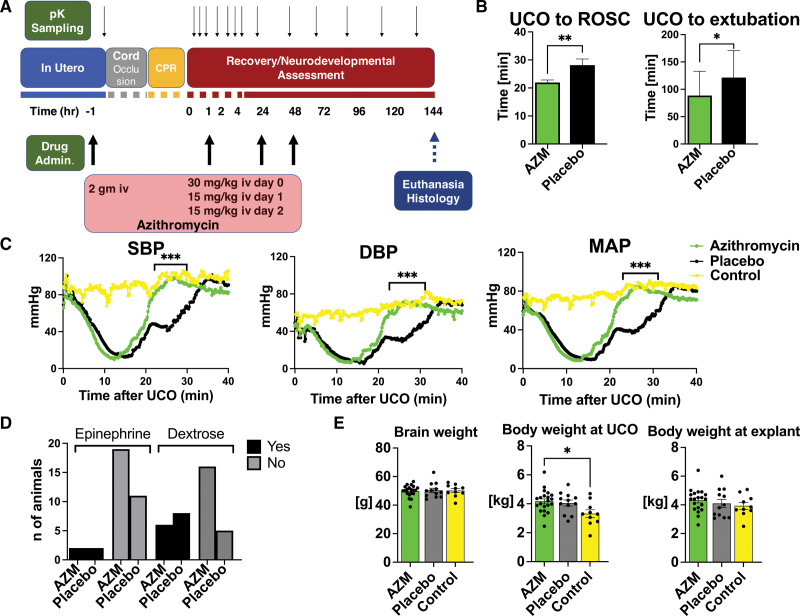
Methods: Ewes and their lambs of both sexes (n=34, 141-143 days) were randomly assigned to receive azithromycin or placebo before delivery as well as postnatally. Lambs were subjected to severe global hypoxia-ischemia utilizing an acute umbilical cord occlusion model. Outcomes were assessed over a 6-day period.
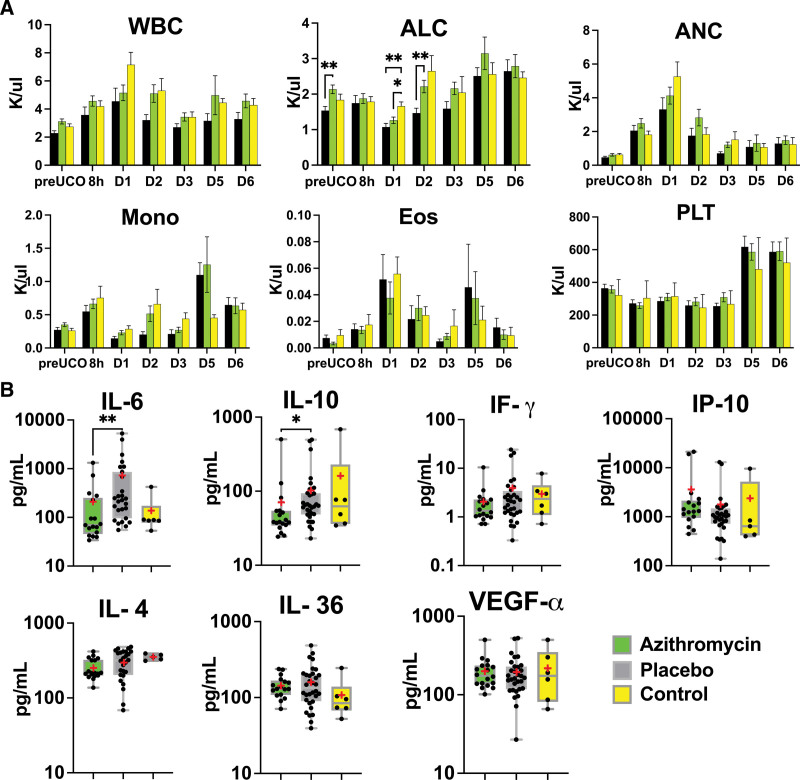
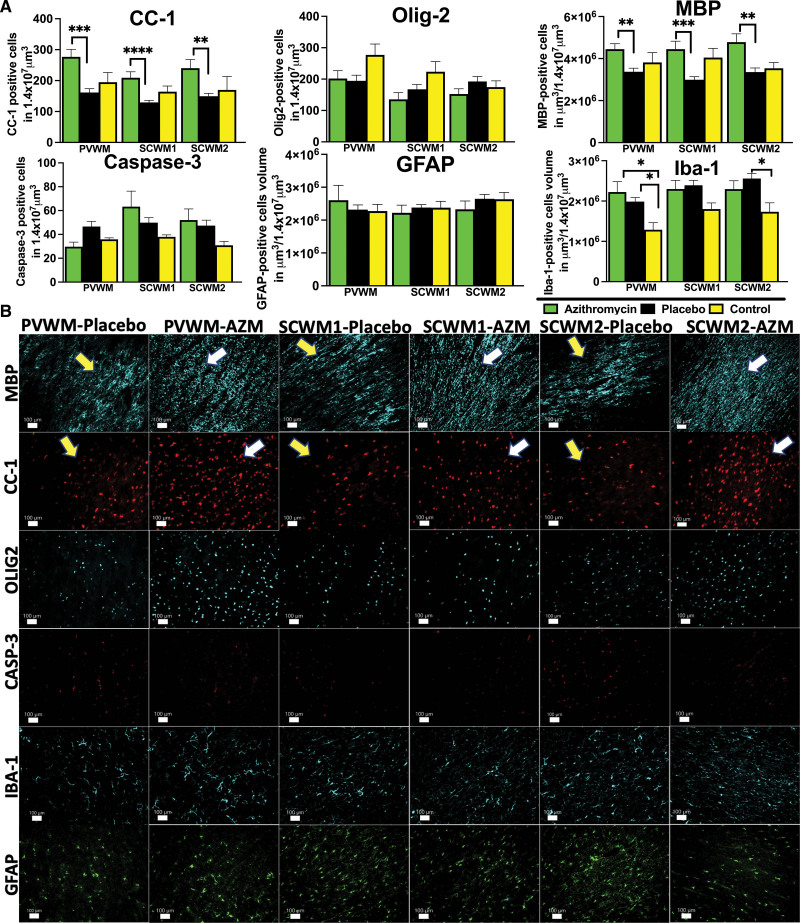
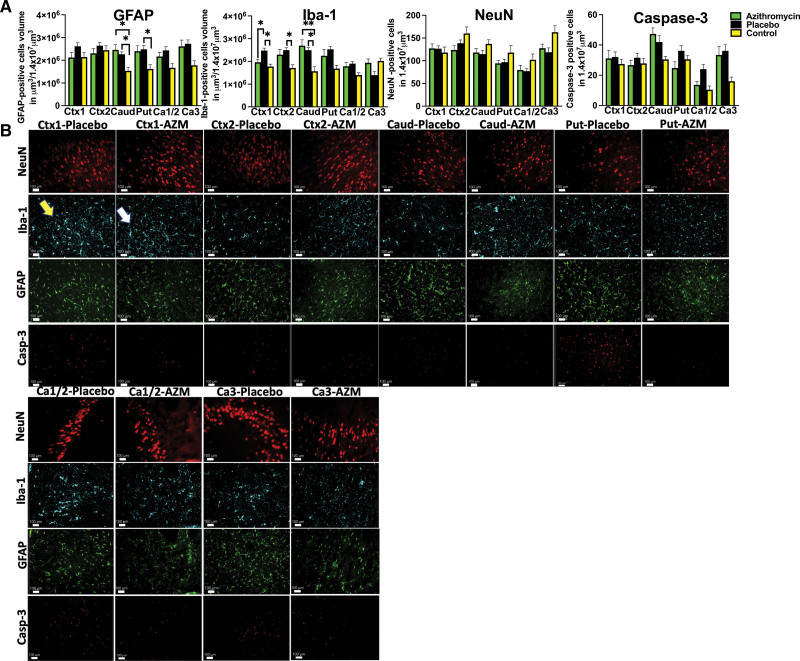
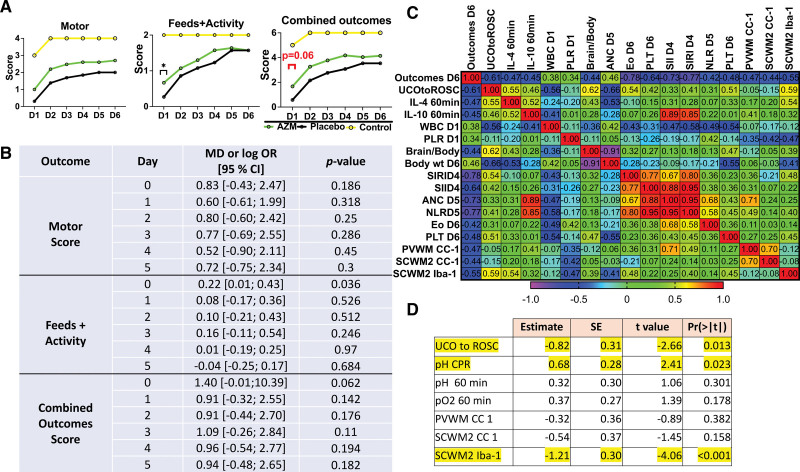
Results: While maternal azithromycin exhibited relatively low placental transfer, azithromycin-treated lambs recovered spontaneous circulation faster following the initiation of cardiopulmonary resuscitation and were extubated sooner. Additionally, peri- and postnatal azithromycin administration was well tolerated, demonstrating a 77-hour plasma elimination half-life, as well as significant accumulation in the brain and other tissues. Azithromycin administration resulted in a systemic immunomodulatory effect, demonstrated by reductions in proinflammatory IL-6 (interleukin-6) levels. Treated lambs exhibited a trend toward improved neurodevelopmental outcomes while histological analysis revealed that azithromycin supported white matter preservation and attenuated inflammation in the cingulate and parasagittal cortex.
Conclusions: Perinatal azithromycin administration enhances neonatal resuscitation, attenuates neuroinflammation, and supports limited improvement of select histological outcomes in an ovine model of hypoxic-ischemic brain injury/encephalopathy.
Keywords: asphyxia; azithromycin; brain hypoxia-ischemia; neonates; ovine model.
Conflict of interest statement
Figures
References
-
- Lee AC, Kozuki N, Blencowe H, Vos T, Bahalim A, Darmstadt GL, Niermeyer S, Ellis M, Robertson NJ, Cousens S, et al. Intrapartum-related neonatal encephalopathy incidence and impairment at regional and global levels for 2010 with trends from 1990. Pediatr Res. 2013;74:50–72. doi: 10.1038/pr.2013.206 - PMC - PubMed
-
- Bhatti A, Kumar P. Systemic effects of perinatal asphyxia. Indian J Pediatr. 2014;81:231–233. doi: 10.1007/s12098-013-1328-9 - PubMed
