

Effects of early postoperative mobilization following gastrointestinal surgery: systematic review and meta-analysis
- PMID: 37846641
- PMCID: PMC10580147
- DOI: 10.1093/bjsopen/zrad102
Effects of early postoperative mobilization following gastrointestinal surgery: systematic review and meta-analysis
Abstract
Background: Early postoperative mobilization is considered a key element of enhanced recovery after surgery protocols. The aim of this study was to summarize the effect of early postoperative mobilization following gastrointestinal operations on patient recovery, mobility, the morbidity rate and duration of hospital stay.
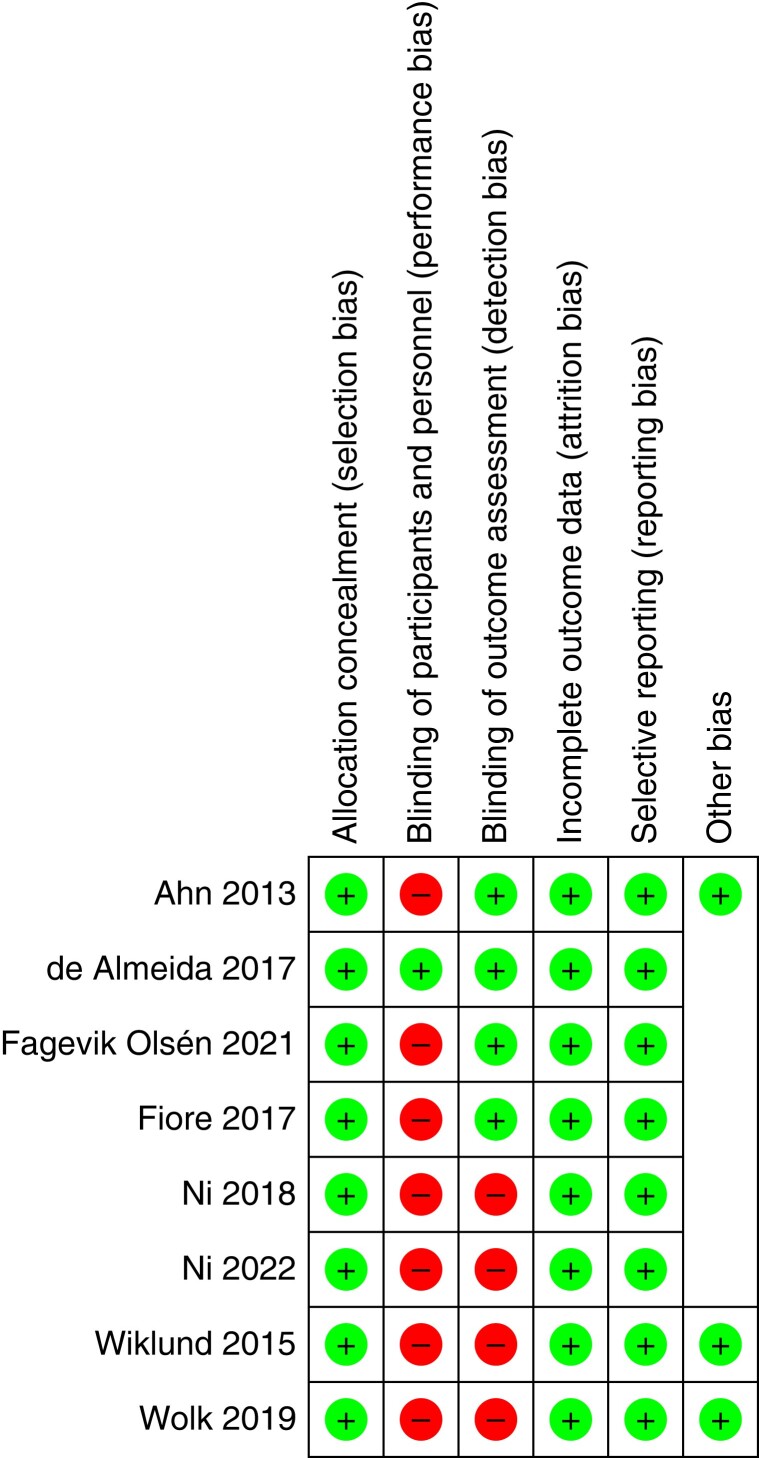
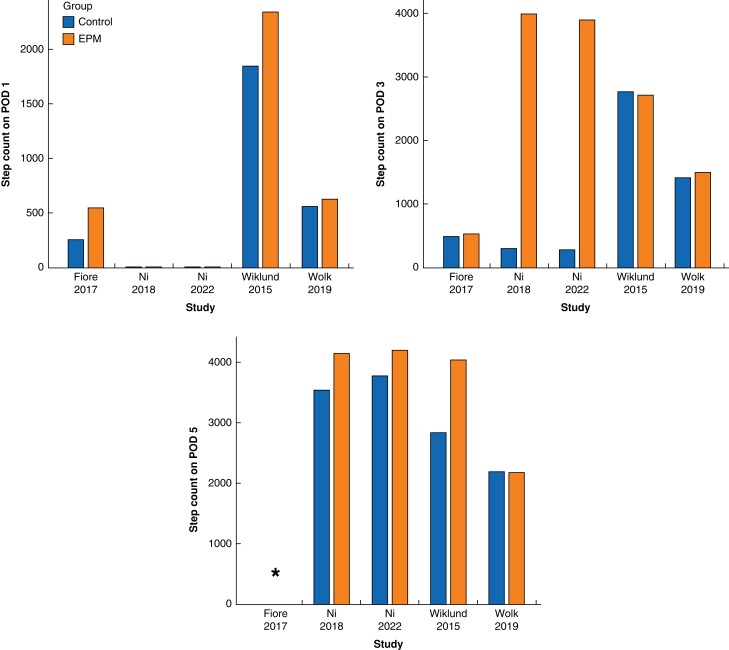
Methods: A systematic literature search was conducted in December, 2022, using PubMed, Web of Science and the Cochrane Central Register of Controlled Trials. Controlled trials reporting the effects of early postoperative mobilization after gastrointestinal surgery were included. The risk of bias was assessed using a modified Downs and Black tool and the Cochrane Collaboration tool for randomized trials. The outcomes of interest were gastrointestinal recovery (defined passage of first flatus or bowel movements), mobility (step count on postoperative day 3), the morbidity rate and duration of hospital stay.
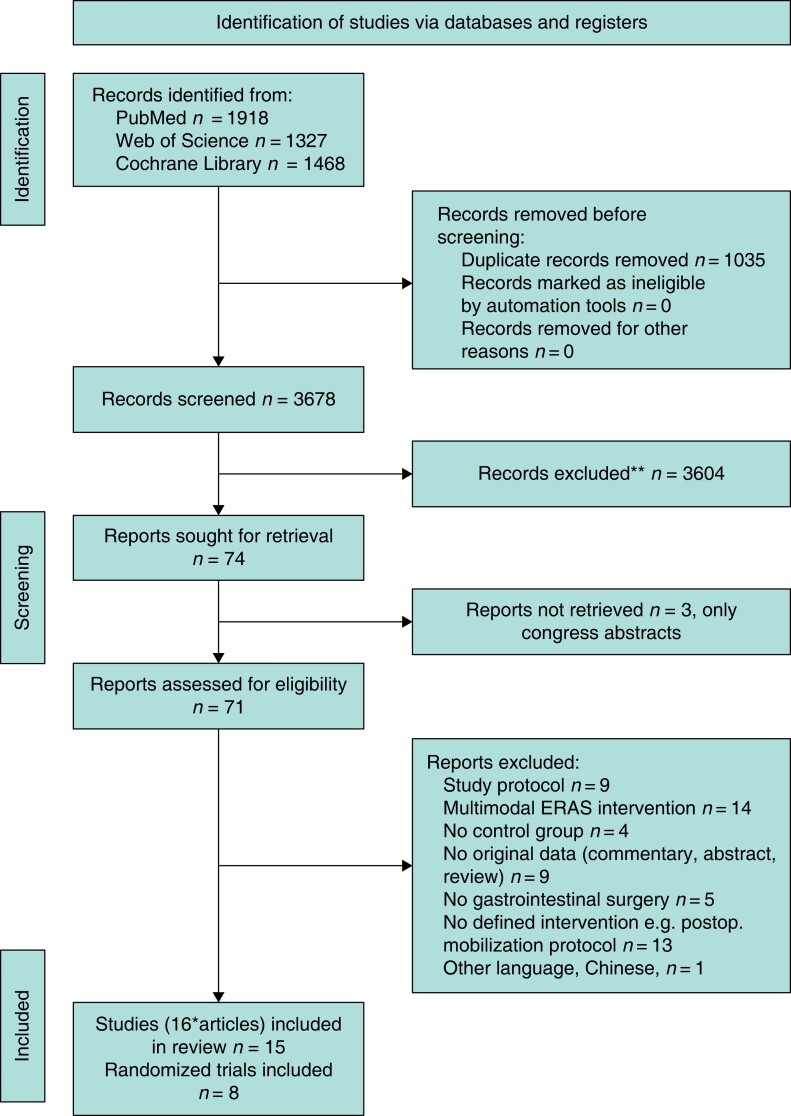
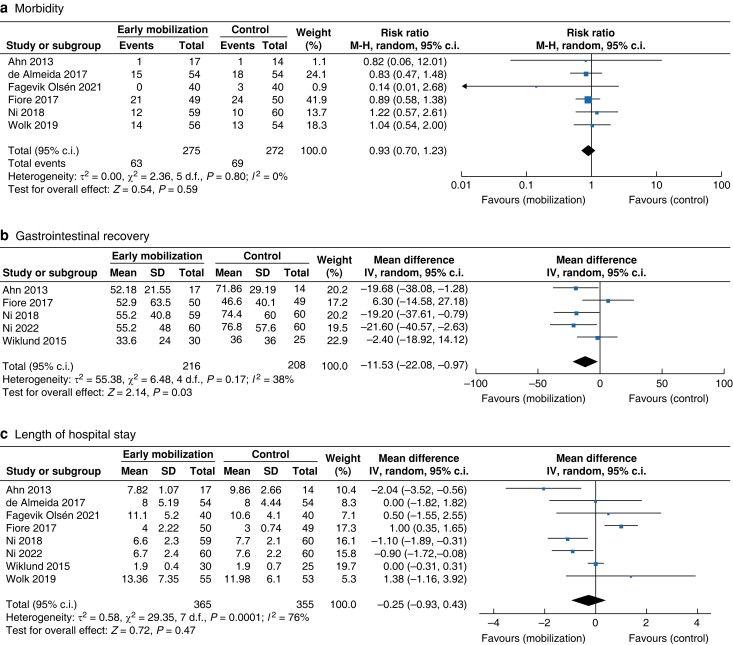
Results: After elimination of duplicates, 3678 records were identified, and 71 full-text articles were screened. Finally, 15 studies (eight RCTs) reporting on 3538 patients were included. Most trials evaluated early postoperative mobilization after different gastrointestinal operations, including upper gastrointestinal (n = 8 studies), hepatopancreatobiliary (n = 10 studies) and colorectal resections (n = 10 studies). The investigated early postoperative mobilization protocols, operative techniques (minimally invasive or open) and outcome parameters were heterogeneous between the studies. Early postoperative mobilization seemed to significantly accelerate clinical gastrointestinal recovery (mean difference, hours: -11.53 (-22.08, -0.97), P = 0.03). However, early postoperative mobilization did not significantly improve the morbidity rate (risk ratio: 0.93 (0.70, 1.23), P = 0.59), postoperative mobility of patients (step count mean difference: 1009 (-803, 2821), P = 0.28) or shorten the duration of hospital stay (mean difference, days: -0.25 (-0.99,0.43), P = 0.47) in randomized trials.
Conclusion: There is a large heterogeneity among the study cohorts, operations and interventions. The available evidence currently does not support specific early postoperative mobilization protocols as an isolated element to further reduce the morbidity rate and duration of hospital stay. Further well-designed trials are required to identify effective early postoperative mobilization protocols.
© The Author(s) 2023. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures

References
-
- Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis Net al. Guidelines for perioperative care in elective colorectal surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations: 2018. World J Surg 2019;43:659–695 - PubMed
-
- Melloul E, Lassen K, Roulin D, Grass F, Perinel J, Adham Met al. Guidelines for perioperative care for pancreatoduodenectomy: Enhanced Recovery After Surgery (ERAS) recommendations 2019. World J Surg 2020;44:2056–2084 - PubMed
-
- Mortensen K, Nilsson M, Slim K, Schäfer M, Mariette C, Braga Met al. Consensus guidelines for enhanced recovery after gastrectomy: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Br J Surg 2014;101:1209–1229 - PubMed
-
- Mata J, Pecorelli N, Kaneva P, Moldoveanu D, Gosselin-Tardiff A, Alhashemi Met al. A mobile device application (app) to improve adherence to an enhanced recovery program for colorectal surgery: a randomized controlled trial. Surg Endosc Interv Tech 2020;34:742–751 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
