

Hyperthyroidism: A Review
- PMID: 37847271
- PMCID: PMC10873132
- DOI: 10.1001/jama.2023.19052
Hyperthyroidism: A Review
Abstract
Importance: Overt hyperthyroidism, defined as suppressed thyrotropin (previously thyroid-stimulating hormone) and high concentration of triiodothyronine (T3) and/or free thyroxine (FT4), affects approximately 0.2% to 1.4% of people worldwide. Subclinical hyperthyroidism, defined as low concentrations of thyrotropin and normal concentrations of T3 and FT4, affects approximately 0.7% to 1.4% of people worldwide. Untreated hyperthyroidism can cause cardiac arrhythmias, heart failure, osteoporosis, and adverse pregnancy outcomes. It may lead to unintentional weight loss and is associated with increased mortality.
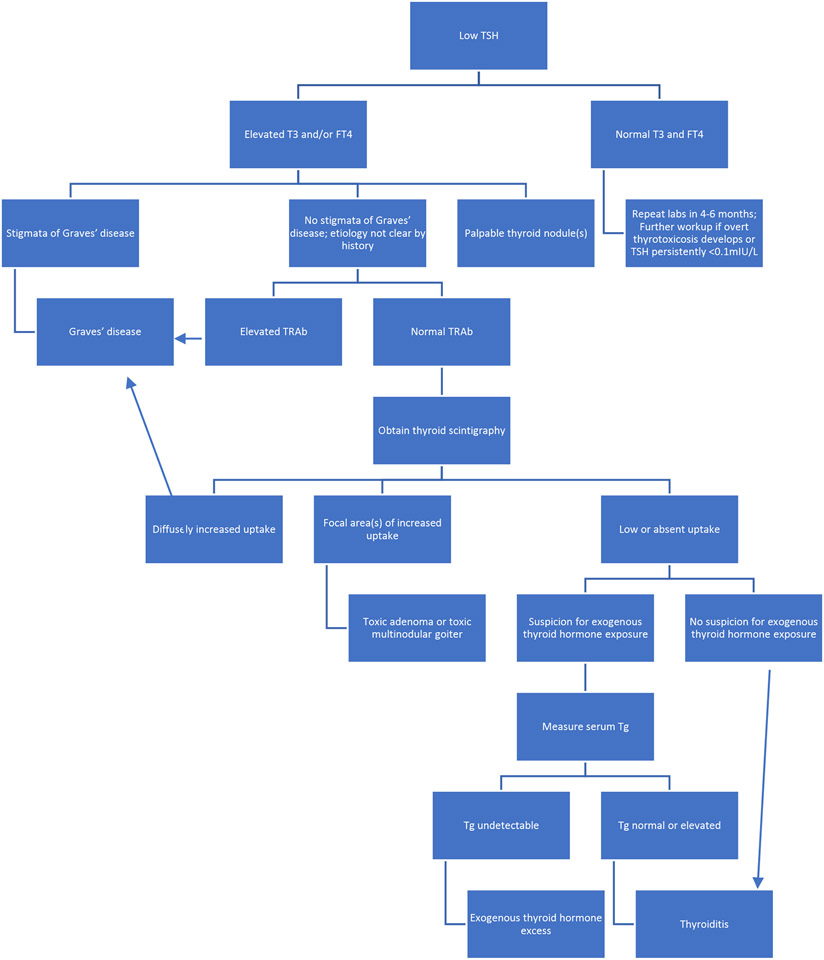
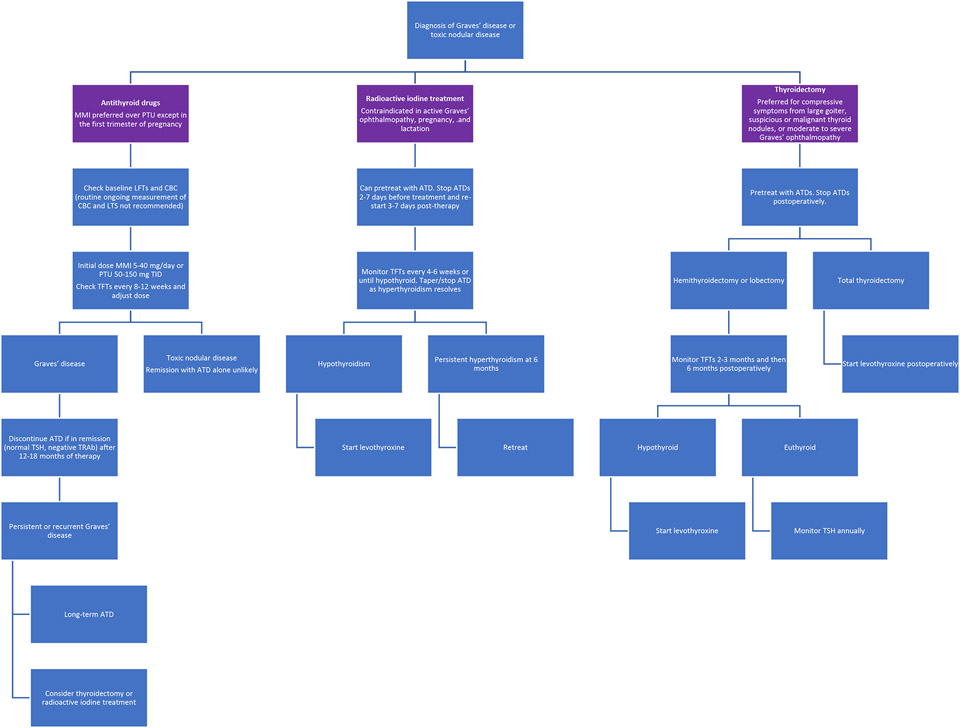
Observations: The most common cause of hyperthyroidism is Graves disease, with a global prevalence of 2% in women and 0.5% in men. Other causes of hyperthyroidism and thyrotoxicosis include toxic nodules and the thyrotoxic phase of thyroiditis. Common symptoms of thyrotoxicosis include anxiety, insomnia, palpitations, unintentional weight loss, diarrhea, and heat intolerance. Patients with Graves disease may have a diffusely enlarged thyroid gland, stare, or exophthalmos on examination. Patients with toxic nodules (ie, in which thyroid nodules develop autonomous function) may have symptoms from local compression of structures in the neck by the thyroid gland, such as dysphagia, orthopnea, or voice changes. Etiology can typically be established based on clinical presentation, thyroid function tests, and thyrotropin-receptor antibody status. Thyroid scintigraphy is recommended if thyroid nodules are present or the etiology is unclear. Thyrotoxicosis from thyroiditis may be observed if symptomatic or treated with supportive care. Treatment options for overt hyperthyroidism from autonomous thyroid nodules or Graves disease include antithyroid drugs, radioactive iodine ablation, and surgery. Treatment for subclinical hyperthyroidism is recommended for patients at highest risk of osteoporosis and cardiovascular disease, such as those older than 65 years or with persistent serum thyrotropin level less than 0.1 mIU/L.
Conclusions and relevance: Hyperthyroidism affects 2.5% of adults worldwide and is associated with osteoporosis, heart disease, and increased mortality. First-line treatments are antithyroid drugs, thyroid surgery, and radioactive iodine treatment. Treatment choices should be individualized and patient centered.
Conflict of interest statement
Figures
Comment in
-
Treatment for Hyperthyroidism During Pregnancy.JAMA. 2024 Mar 5;331(9):798. doi: 10.1001/jama.2023.28197. JAMA. 2024. PMID: 38441590 No abstract available.
References
-
- Laurberg P, Pedersen KM, Vestergaard H, Sigurdsson G. High incidence of multinodular toxic goitre in the elderly population in a low iodine intake area vs. high incidence of Graves’ disease in the young in a high iodine intake area: comparative surveys of thyrotoxicosis epidemiology in East-Jutland Denmark and Iceland. J Intern Med. 1991;229(5):415–20. doi: 10.1111/j.1365-2796.1991.tb00368.x - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
