

Prediction model of no-response before the first transarterial chemoembolization for hepatocellular carcinoma: TACF score
- PMID: 37847433
- PMCID: PMC10581972
- DOI: 10.1007/s12672-023-00803-2
Prediction model of no-response before the first transarterial chemoembolization for hepatocellular carcinoma: TACF score
Abstract
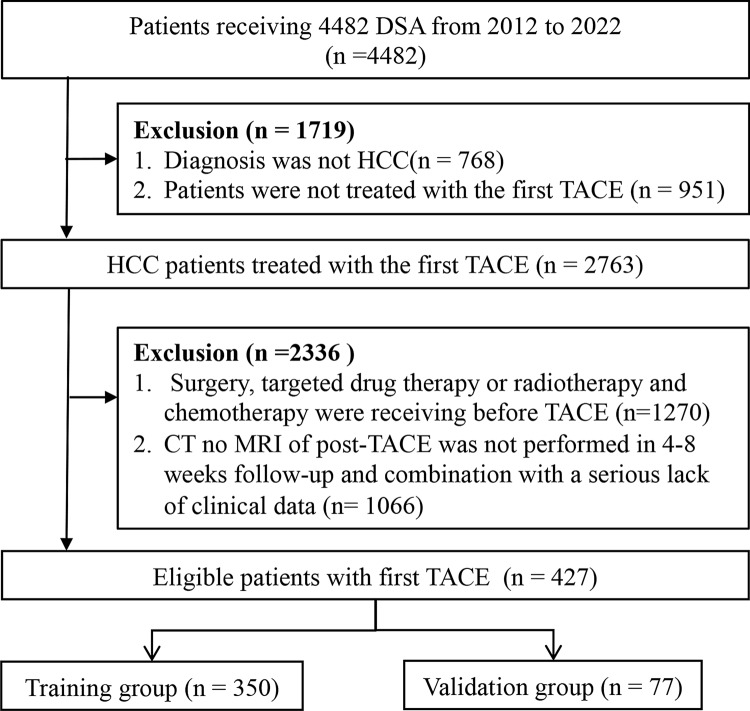
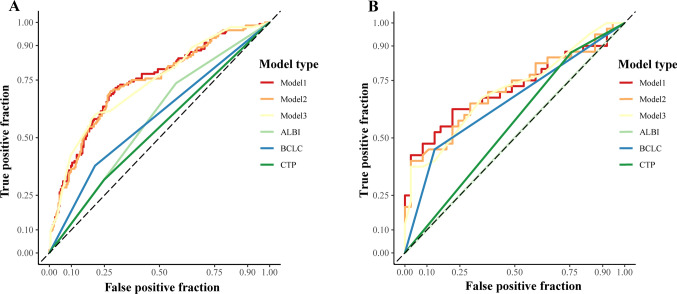
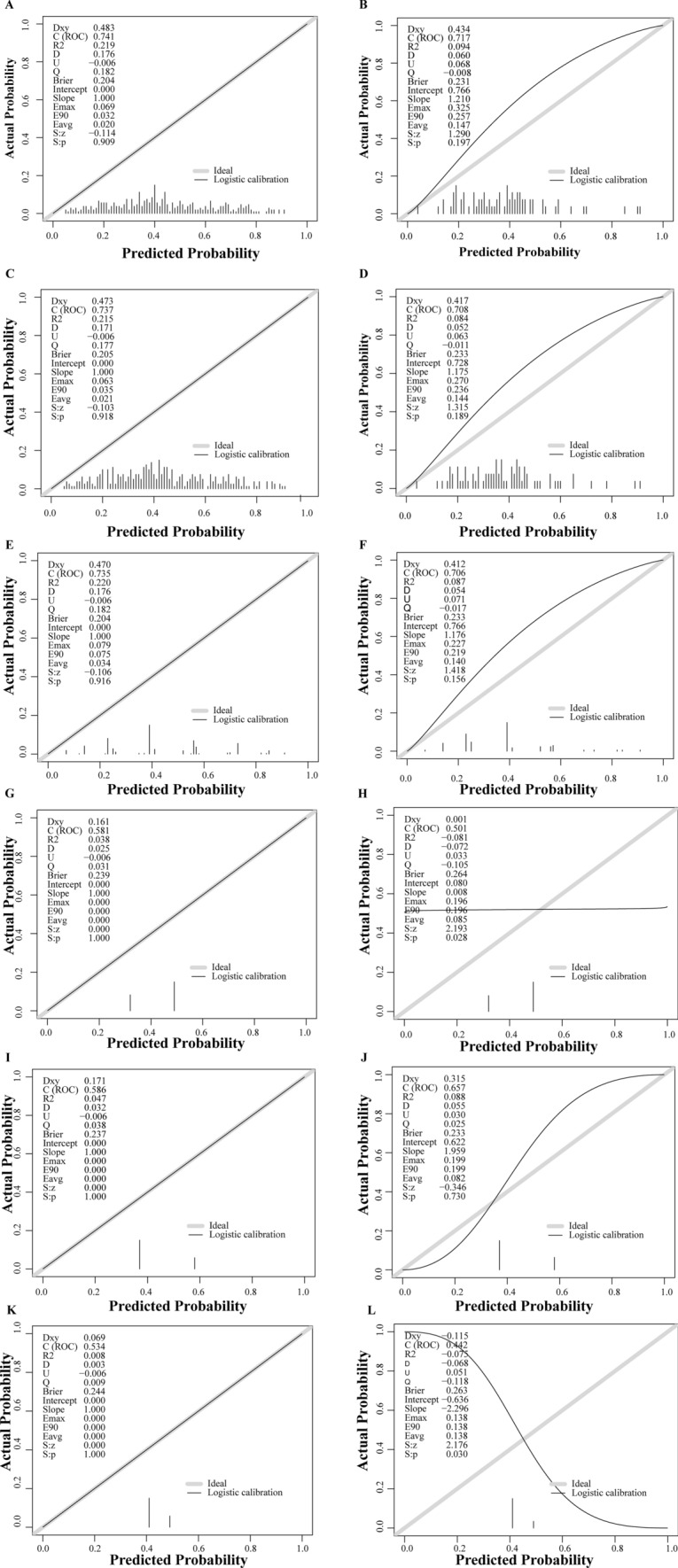
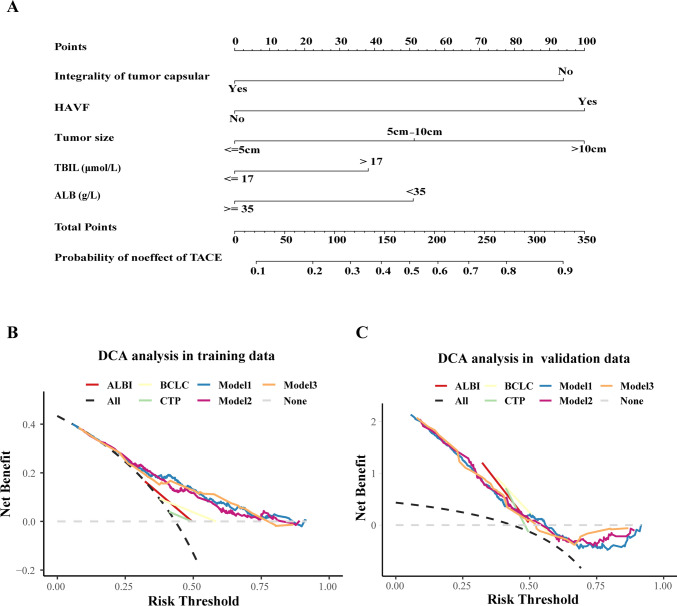
Previous clinic models for patients with hepatocellular carcinoma (HCC) receiving transarterial chemoembolization (TACE) mainly focused on the overall survival, whereas a simple-to-use tool for predicting the response to the first TACE and the management of risk classification before TACE are lacking. Our aim was to develop a scoring system calculated manually for these patients. A total of 437 patients with hepatocellular carcinoma (HCC) who underwent TACE treatment were carefully selected for analysis. They were then randomly divided into two groups: a training group comprising 350 patients and a validation group comprising 77 patients. Furthermore, 45 HCC patients who had recently undergone TACE treatment been included in the study to validate the model's efficacy and applicability. The factors selected for the predictive model were comprehensively based on the results of the LASSO, univariate and multivariate logistic regression analyses. The discrimination, calibration ability and clinic utility of models were evaluated in both the training and validation groups. A prediction model incorporated 3 objective imaging characteristics and 2 indicators of liver function. The model showed good discrimination, with AUROCs of 0.735, 0.706 and 0.884 and in the training group and validation groups, and good calibration. The model classified the patients into three groups based on the calculated score, including low risk, median risk and high-risk groups, with rates of no response to TACE of 26.3%, 40.2% and 76.8%, respectively. We derived and validated a model for predicting the response of patients with HCC before receiving the first TACE that had adequate performance and utility. This model may be a useful and layered management tool for patients with HCC undergoing TACE.
Keywords: First response; Hepatocellular carcinoma; Individual prediction; Transarterial chemoembolization.
© 2023. Springer Science+Business Media, LLC.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Bruix J, Reig M, Sherman M. Evidence-based diagnosis, staging, and treatment of patients with hepatocellular carcinoma. Gastroenterology. 2016;150:835–853. - PubMed
-
- Marrero JA, Kulik LM, Sirlin CB, Zhu AX, Finn RS, Abecassis MM, Roberts LR, Heimbach JK. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American association for the study of liver diseases. Hepatology. 2018;68:723–750. - PubMed
-
- Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology. 2003;37:429–442. - PubMed
-
- Maesaka K, Sakamori R, Yamada R, Tahata Y, Urabe A, Shigekawa M, Kodama T, Hikita H, Tatsumi T, Takehara T. Hypovascular hepatic nodules as a predictive factor for transcatheter arterial chemoembolization refractoriness in hepatocellular carcinoma. Hepatol Res. 2020;50:365–373. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous