

Effects of CPAP and FiO2 on respiratory effort and lung stress in early COVID-19 pneumonia: a randomized, crossover study
- PMID: 37847454
- PMCID: PMC10581975
- DOI: 10.1186/s13613-023-01202-0
Effects of CPAP and FiO2 on respiratory effort and lung stress in early COVID-19 pneumonia: a randomized, crossover study
Abstract
Background: in COVID-19 acute respiratory failure, the effects of CPAP and FiO2 on respiratory effort and lung stress are unclear. We hypothesize that, in the compliant lungs of early Sars-CoV-2 pneumonia, the application of positive pressure through Helmet-CPAP may not decrease respiratory effort, and rather worsen lung stress and oxygenation when compared to higher FiO2 delivered via oxygen masks.
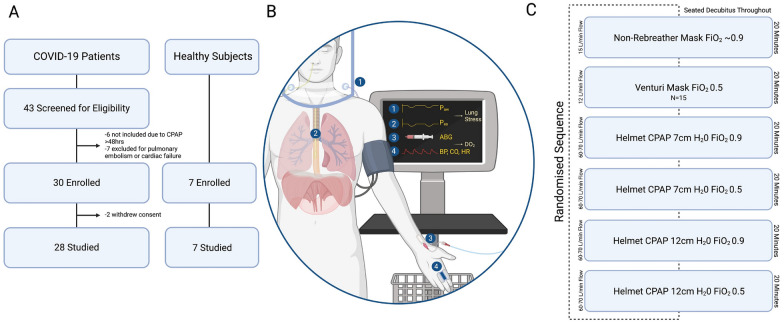
Methods: In this single-center (S.Luigi Gonzaga University-Hospital, Turin, Italy), randomized, crossover study, we included patients receiving Helmet-CPAP for early (< 48 h) COVID-19 pneumonia without additional cardiac or respiratory disease. Healthy subjects were included as controls. Participants were equipped with an esophageal catheter, a non-invasive cardiac output monitor, and an arterial catheter. The protocol consisted of a random sequence of non-rebreather mask (NRB), Helmet-CPAP (with variable positive pressure and FiO2) and Venturi mask (FiO2 0.5), each delivered for 20 min. Study outcomes were changes in respiratory effort (esophageal swing), total lung stress (dynamic + static transpulmonary pressure), gas-exchange and hemodynamics.
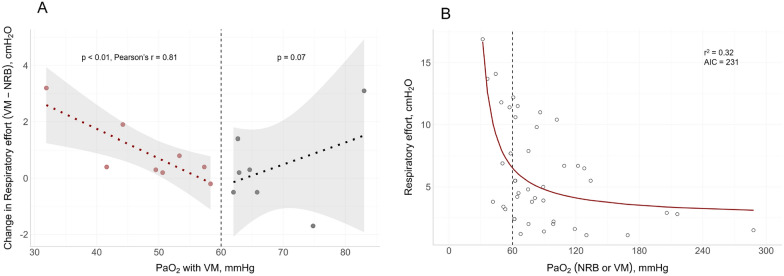
Results: We enrolled 28 COVID-19 patients and 7 healthy controls. In all patients, respiratory effort increased from NRB to Helmet-CPAP (5.0 ± 3.7 vs 8.3 ± 3.9 cmH2O, p < 0.01). However, Helmet's pressure decreased by a comparable amount during inspiration (- 3.1 ± 1.0 cmH2O, p = 0.16), therefore dynamic stress remained stable (p = 0.97). Changes in static and total lung stress from NRB to Helmet-CPAP were overall not significant (p = 0.07 and p = 0.09, respectively), but showed high interpatient variability, ranging from - 4.5 to + 6.1 cmH2O, and from - 5.8 to + 5.7 cmH2O, respectively. All findings were confirmed in healthy subjects, except for an increase in dynamic stress (p < 0.01). PaO2 decreased from NRB to Helmet-CPAP with FiO2 0.5 (107 ± 55 vs 86 ± 30 mmHg, p < 0.01), irrespective of positive pressure levels (p = 0.64). Conversely, with Helmet's FiO2 0.9, PaO2 increased (p < 0.01), but oxygen delivery remained stable (p = 0.48) as cardiac output decreased (p = 0.02). When PaO2 fell below 60 mmHg with VM, respiratory effort increased proportionally (p < 0.01, r = 0.81).
Conclusions: In early COVID-19 pneumonia, Helmet-CPAP increases respiratory effort without altering dynamic stress, while the effects upon static and total stress are variable, requiring individual assessment. Oxygen masks with higher FiO2 provide better oxygenation with lower respiratory effort. Trial registration Retrospectively registered (13-May-2021): clinicaltrials.gov (NCT04885517), https://clinicaltrials.gov/ct2/show/NCT04885517 .
Keywords: COVID-19; Gas-exchange; Helmet-CPAP; Hemodynamics; Lung stress; Non-rebreather mask; Respiratory effort; Respiratory failure; Venturi mask.
© 2023. La Société de Réanimation de Langue Francaise = The French Society of Intensive Care (SRLF).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Perkins GD, Ji C, Connolly BA, Couper K, Lall R, Baillie JK, et al. Effect of noninvasive respiratory strategies on intubation or mortality among patients with acute hypoxemic respiratory failure and COVID-19: the recovery-rs randomized clinical trial. JAMA. 2022;327:546–558. doi: 10.1001/jama.2022.0028. - DOI - PMC - PubMed
-
- Grieco DL, Menga LS, Cesarano M, Rosà T, Spadaro S, Bitondo MM, et al. Effect of helmet noninvasive ventilation vs high-flow nasal oxygen on days free of respiratory support in patients with COVID-19 and moderate to severe hypoxemic respiratory failure: the HENIVOT randomized clinical trial. JAMA. 2021;325:1731–1743. doi: 10.1001/jama.2021.4682. - DOI - PMC - PubMed
-
- Sakuraya M, Okano H, Masuyama T, Kimata S, Hokari S. Efficacy of non-invasive and invasive respiratory management strategies in adult patients with acute hypoxaemic respiratory failure: a systematic review and network meta-analysis. Crit Care. 2021;25:414. doi: 10.1186/s13054-021-03835-8. - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
