

[Finite element analysis of five internal fixation modes in treatment of Day type Ⅱ crescent fracture dislocation of pelvis]
- PMID: 37848314
- PMCID: PMC10581872
- DOI: 10.7507/1002-1892.202306043
[Finite element analysis of five internal fixation modes in treatment of Day type Ⅱ crescent fracture dislocation of pelvis]
Abstract
Objective: To compare the biomechanical differences among the five internal fixation modes in treatment of Day type Ⅱ crescent fracture dislocation of pelvis (CFDP), and find an internal fixation mode which was the most consistent with mechanical principles.
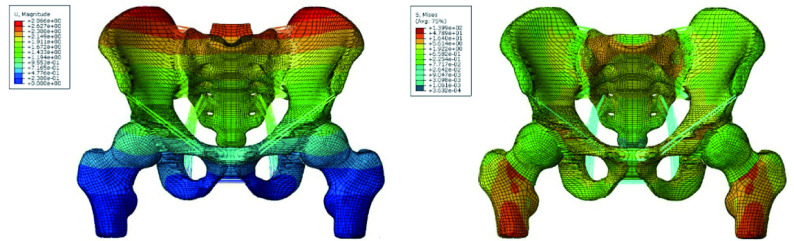
Methods: Based on the pelvic CT data of a healthy adult male volunteer, a Day type Ⅱ CFDP finite element model was established by using Mimics 17.0, ANSYS 12.0-ICEM, Abaqus 2020, and SolidWorks 2012 softwares. After verifying the validity of the finite element model by comparing the anatomical parameters with the three-dimensional reconstruction model and the mechanical validity verification, the fracture and dislocated joint of models were fixed with S 1 sacroiliac screw combined with 1 LC-Ⅱ screw (S 1+LC-Ⅱ group), S 1 sacroiliac screw combined with 2 LC-Ⅱ screws (S 1+2LC-Ⅱ group), S 1 sacroiliac screw combined with 2 posterior iliac screws (S 1+2PIS group), S 1 and S 2 sacroiliac screws combined with 1 LC-Ⅱ screw (S 1+S 2+LC-Ⅱ group), S 2-alar-iliac (S 2AI) screw combined with 1 LC-Ⅱ screw (S 2AI+LC-Ⅱ group), respectively. After each internal fixation model was loaded with a force of 600 N in the standing position, the maximum displacement of the crescent fracture fragments, the maximum stress of the internal fixation (the maximum stress of the screw at the ilium fracture and the maximum stress of the screw at the sacroiliac joint), sacroiliac joint displacement, and bone stress distribution around internal fixation were observed in 5 groups.
Results: The finite element model in this study has been verified to be effective. After loading 600 N stress, there was a certain displacement of the crescent fracture of pelvis in each internal fixation model, among which the S 1+LC-Ⅱ group was the largest, the S 1+2LC-Ⅱ group and the S 1+2PIS group were the smallest. The maximum stress of the internal fixation mainly concentrated at the sacroiliac joint and the fracture line of crescent fracture. The maximum stress of the screw at the sacroiliac joint was the largest in the S 1+LC-Ⅱ group and the smallest in the S 2AI+LC-Ⅱ group. The maximum stress of the screw at the ilium fracture was the largest in the S 1+2PIS group and the smallest in the S 1+2LC-Ⅱ group. The displacement of the sacroiliac joint was the largest in the S 1+LC-Ⅱ group and the smallest in the S 1+S 2+LC-Ⅱ group. In each internal fixation model, the maximum stress around the sacroiliac screws concentrated on the contact surface between the screw and the cortical bone, the maximum stress around the screws at the iliac bone concentrated on the cancellous bone of the fracture line, and the maximum stress around the S 2AI screw concentrated on the cancellous bone on the iliac side. The maximum bone stress around the screws at the sacroiliac joint was the largest in the S 1+LC-Ⅱ group and the smallest in the S 2AI+LC-Ⅱ group. The maximum bone stress around the screws at the ilium was the largest in the S 1+2PIS group and the smallest in the S 1+LC-Ⅱ group.
Conclusion: For the treatment of Day type Ⅱ CFDP, it is recommended to choose S 1 sacroiliac screw combined with 1 LC-Ⅱ screw for internal fixation, which can achieve a firm fixation effect without increasing the number of screws.
目的: 采用有限元分析比较5种内固定方式治疗Day Ⅱ型骨盆新月形骨折脱位(crescent fracture dislocation of pelvis,CFDP)的生物力学差异,探讨最符合力学原理的内固定方式。.
方法: 取1名健康成年男性志愿者骨盆CT数据,利用Mimics17.0、ANSYS 12.0-ICEM、Abaqus 2020、SolidWorks 2012软件建立Day Ⅱ型CFDP有限元模型,通过与三维重建模型解剖参数比较以及力学有效性验证来评估模型有效性后,分别采用S 1骶髂螺钉+1枚LC-Ⅱ螺钉(S 1+LC-Ⅱ组)、S 1骶髂螺钉+2枚LC-Ⅱ螺钉(S 1+2LC-Ⅱ组)、S 1骶髂螺钉+2枚髂骨后螺钉(posterior iliac screw,PIS)(S 1+2PIS组)、S 1骶髂螺钉+S 2骶髂螺钉+1枚LC-Ⅱ螺钉(S 1+S 2+LC-Ⅱ组)、经第2骶椎髂骨翼(S 2-alar-iliac,S 2AI)螺钉+1枚LC-Ⅱ螺钉(S 2AI+LC-Ⅱ组)固定骨折及脱位关节。对各内固定模型站立位下加载600 N应力后,观测5组内固定模型中新月形骨折块最大位移、内固定最大应力(髂骨骨折处螺钉最大应力及骶髂关节处螺钉最大应力)、骶髂关节位移、内固定周围骨应力分布。.
结果: 经验证构建的有限元模型有效。加载600 N应力后,各内固定模型新月形骨折块均存在一定位移,其中S 1+LC-Ⅱ组最大,S 1+2LC-Ⅱ组及S 1+2PIS组最小;内固定最大应力主要集中在骶髂关节和新月形骨折线处,其中骶髂关节处螺钉最大应力S 1+LC-Ⅱ组最大、S 2AI+LC-Ⅱ组最小,髂骨骨折处螺钉最大应力S 1+2PIS组最大、S 1+2LC-Ⅱ组最小。骶髂关节位移 S 1+LC-Ⅱ组最大、S 1+S 2-LC-Ⅱ组最小。各内固定模型中骶髂螺钉周围最大应力集中在螺钉与皮质骨的接触面,髂骨处螺钉集中于骨折线松质骨处,S 2AI螺钉集中在髂骨侧松质骨内。骶髂关节处螺钉周围骨最大应力S 1+LC-Ⅱ组最大、S 2AI+LC-Ⅱ组最小,髂骨处螺钉周围骨最大应力S 1+2PIS组最大、S 1+LC-Ⅱ组最小。.
结论: Day Ⅱ型CFDP治疗宜选择S 1骶髂螺钉联合1枚LC-Ⅱ螺钉内固定,在不增加螺钉数量情况下即可达牢固固定效果。.
Keywords: Crescent fracture dislocation of pelvis; finite element analysis; internal fixation; screw.
Conflict of interest statement
利益冲突 在课题研究和文章撰写过程中不存在利益冲突;经费支持没有影响文章观点和对研究数据客观结果的统计分析及其报道
Figures






Similar articles
-
Biomechanical performance evaluation of S2AI combine with LC-2 screw for day II pelvic crescent fracture dislocation via finite element analysis.Sci Rep. 2025 May 14;15(1):16765. doi: 10.1038/s41598-025-00156-6. Sci Rep. 2025. PMID: 40368891 Free PMC article.
-
A novel percutaneous crossed screws fixation in treatment of Day type II crescent fracture-dislocation: A finite element analysis.J Orthop Translat. 2019 Sep 5;20:37-46. doi: 10.1016/j.jot.2019.08.002. eCollection 2020 Jan. J Orthop Translat. 2019. PMID: 31908932 Free PMC article.
-
Biomechanical study of anterior and posterior pelvic rings using pedicle screw fixation for Tile C1 pelvic fractures: Finite element analysis.PLoS One. 2022 Aug 25;17(8):e0273351. doi: 10.1371/journal.pone.0273351. eCollection 2022. PLoS One. 2022. PMID: 36006983 Free PMC article.
-
Finite element analysis of sacral-alar-iliac screw fixation for sacroiliac joint dislocation.J Orthop Res. 2023 Aug;41(8):1821-1830. doi: 10.1002/jor.25525. Epub 2023 Jan 31. J Orthop Res. 2023. PMID: 36691867
-
[Application of second sacral alar-iliac screw technique for reconstruction of spinopelvic stability].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018 Jun 15;32(6):764-768. doi: 10.7507/1002-1892.201711124. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018. PMID: 29905058 Free PMC article. Review. Chinese.
References
-
- Day AC, Kinmont C, Bircher MD, et al Crescent fracture-dislocation of the sacroiliac joint: a functional classification. J Bone Joint Surg (Br) 2007;89(5):651–658. - PubMed
-
- 冯永增, 董效禹, 项光恒, 等 微创经皮交叉螺钉内固定治疗Day Ⅱ型骨盆新月形骨折脱位的临床疗效研究. 中国现代医生. 2020;58(34):80–84.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical