

Interactions of platelets with obesity in relation to lung cancer risk in the UK Biobank cohort
- PMID: 37848891
- PMCID: PMC10580651
- DOI: 10.1186/s12931-023-02561-9
Interactions of platelets with obesity in relation to lung cancer risk in the UK Biobank cohort
Abstract
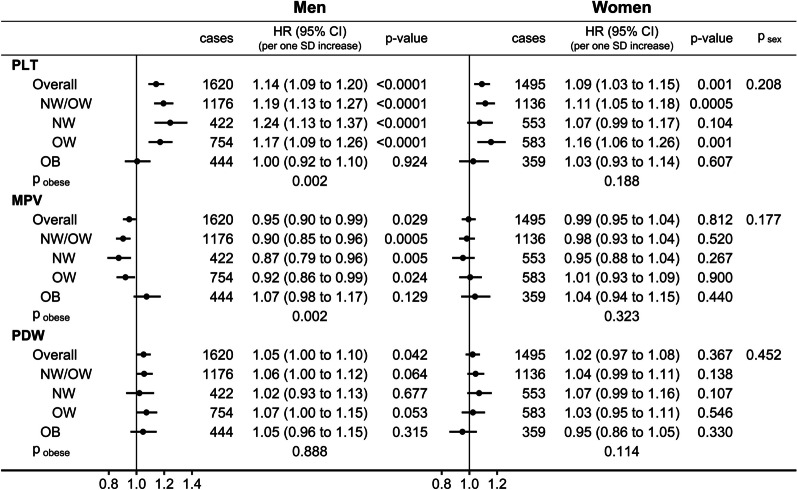
Background: Platelet count (PLT) is associated positively with lung cancer risk but has a more complex association with body mass index (BMI), positive only in women (mainly never smokers) and inverse in men (mainly ever smokers), raising the question whether platelets interact with obesity in relation to lung cancer risk. Prospective associations of platelet size (an index of platelet maturity and activity) with lung cancer risk are unclear.
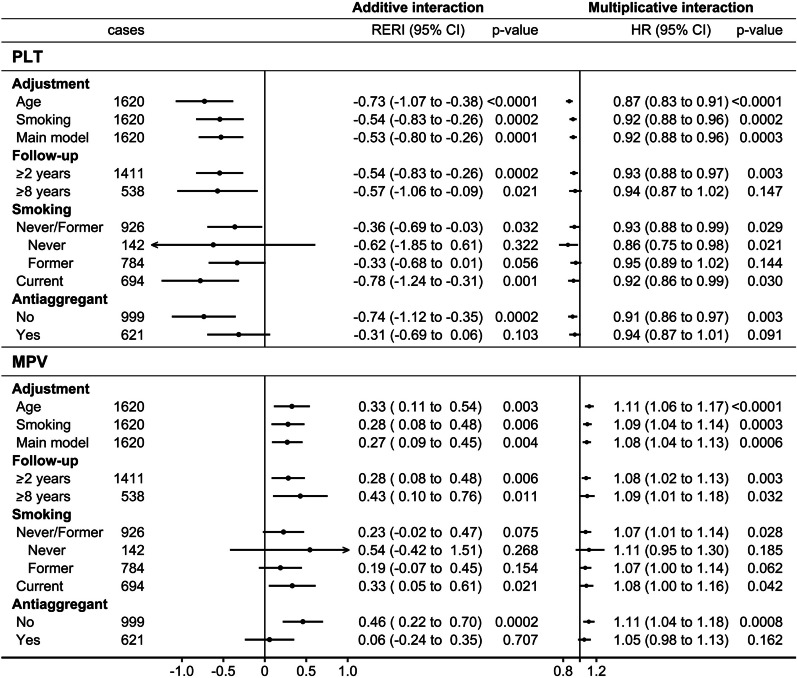
Methods: We examined the associations of PLT, mean platelet volume (MPV), and platelet distribution width (PDW) (each individually, per one standard deviation increase) with lung cancer risk in UK Biobank men and women using multivariable Cox proportional hazards models adjusted for BMI and covariates. We calculated Relative Excess Risk from Interaction (RERI) with obese (BMI ≥ 30 kg/m2), dichotomising platelet parameters at ≥ median (sex-specific), and multiplicative interactions with BMI (continuous scale). We examined heterogeneity according to smoking status (never, former, current smoker) and antiaggregant/anticoagulant use (no/yes).
Results: During a mean follow-up of 10.4 years, 1620 lung cancers were ascertained in 192,355 men and 1495 lung cancers in 218,761 women. PLT was associated positively with lung cancer risk in men (hazard ratio HR = 1.14; 95% confidence interval (CI): 1.09-1.20) and women (HR = 1.09; 95%CI: 1.03-1.15) but interacted inversely with BMI only in men (RERI = - 0.53; 95%CI: - 0.80 to - 0.26 for high-PLT-obese; HR = 0.92; 95%CI = 0.88-0.96 for PLT*BMI). Only in men, MPV was associated inversely with lung cancer risk (HR = 0.95; 95%CI: 0.90-0.99) and interacted positively with BMI (RERI = 0.27; 95%CI = 0.09-0.45 for high-MPV-obese; HR = 1.08; 95%CI = 1.04-1.13 for MPV*BMI), while PDW was associated positively (HR = 1.05; 95%CI: 1.00-1.10), with no evidence for interactions. The associations with PLT were consistent by smoking status, but MPV was associated inversely only in current smokers and PDW positively only in never/former smokers. The interactions with BMI were retained for at least eight years of follow-up and were consistent by smoking status but were attenuated in antiaggregant/anticoagulant users.
Conclusions: In men, PLT was associated positively and MPV inversely with lung cancer risk and these associations appeared hindered by obesity. In women, only PLT was associated positively, with little evidence for interaction with obesity.
Keywords: Interaction; Lung cancer; MPV; Obesity; PDW; Platelet count.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Allometric fat mass index and alanine aminotransferase attenuate the associations of platelet parameters with lung cancer risk.Sci Rep. 2024 Nov 1;14(1):26318. doi: 10.1038/s41598-024-78281-x. Sci Rep. 2024. PMID: 39487349 Free PMC article.
-
Prospective associations of leucocyte subtypes and obesity with the risk of developing cutaneous malignant melanoma in the UK Biobank cohort.BMC Cancer. 2024 May 23;24(1):625. doi: 10.1186/s12885-024-12344-0. BMC Cancer. 2024. PMID: 38783251 Free PMC article.
-
Sex differences in the associations of body size and body shape with platelets in the UK Biobank cohort.Biol Sex Differ. 2023 Feb 22;14(1):12. doi: 10.1186/s13293-023-00494-y. Biol Sex Differ. 2023. PMID: 36814334 Free PMC article.
-
Interactions of obesity, body shape, diabetes and sex steroids with respect to prostate cancer risk in the UK Biobank cohort.Cancer Med. 2024 Feb;13(3):e6918. doi: 10.1002/cam4.6918. Epub 2024 Jan 17. Cancer Med. 2024. PMID: 38234143 Free PMC article.
-
Platelet abnormalities in autoimmune thyroid diseases: A systematic review and meta-analysis.Front Immunol. 2022 Dec 22;13:1089469. doi: 10.3389/fimmu.2022.1089469. eCollection 2022. Front Immunol. 2022. PMID: 36618418 Free PMC article.
Cited by
-
Associations of leucocyte subtypes and platelet parameters with kidney cancer risk in the UK Biobank cohort.J Inflamm (Lond). 2025 Aug 11;22(1):31. doi: 10.1186/s12950-025-00458-6. J Inflamm (Lond). 2025. PMID: 40790491 Free PMC article.
-
Allometric fat mass index and alanine aminotransferase attenuate the associations of platelet parameters with lung cancer risk.Sci Rep. 2024 Nov 1;14(1):26318. doi: 10.1038/s41598-024-78281-x. Sci Rep. 2024. PMID: 39487349 Free PMC article.
-
Prospective associations of leucocyte subtypes and obesity with the risk of developing cutaneous malignant melanoma in the UK Biobank cohort.BMC Cancer. 2024 May 23;24(1):625. doi: 10.1186/s12885-024-12344-0. BMC Cancer. 2024. PMID: 38783251 Free PMC article.
References
-
- Bailey SE, Ukoumunne OC, Shephard EA, Hamilton W. Clinical relevance of thrombocytosis in primary care: a prospective cohort study of cancer incidence using English electronic medical records and cancer registry data. Br J Gen Pract. 2017;67(659):e405–e413. doi: 10.3399/bjgp17X691109. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
