

Quantifying the Expanding Landscape of Clinical Actionability for Patients with Cancer
- PMID: 37849038
- PMCID: PMC10784742
- DOI: 10.1158/2159-8290.CD-23-0467
Quantifying the Expanding Landscape of Clinical Actionability for Patients with Cancer
Abstract
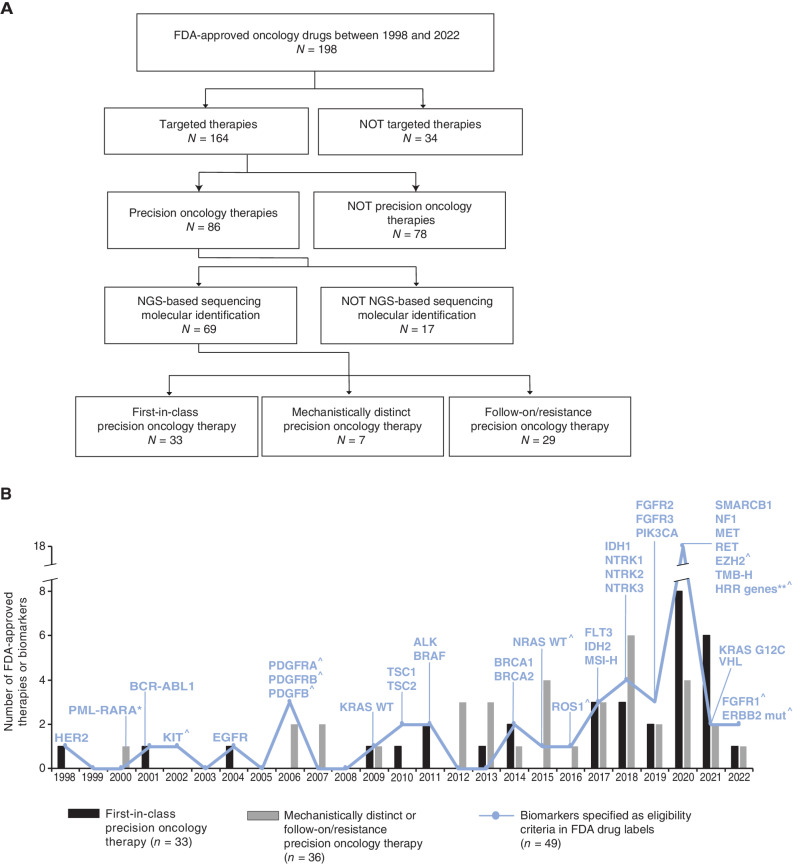
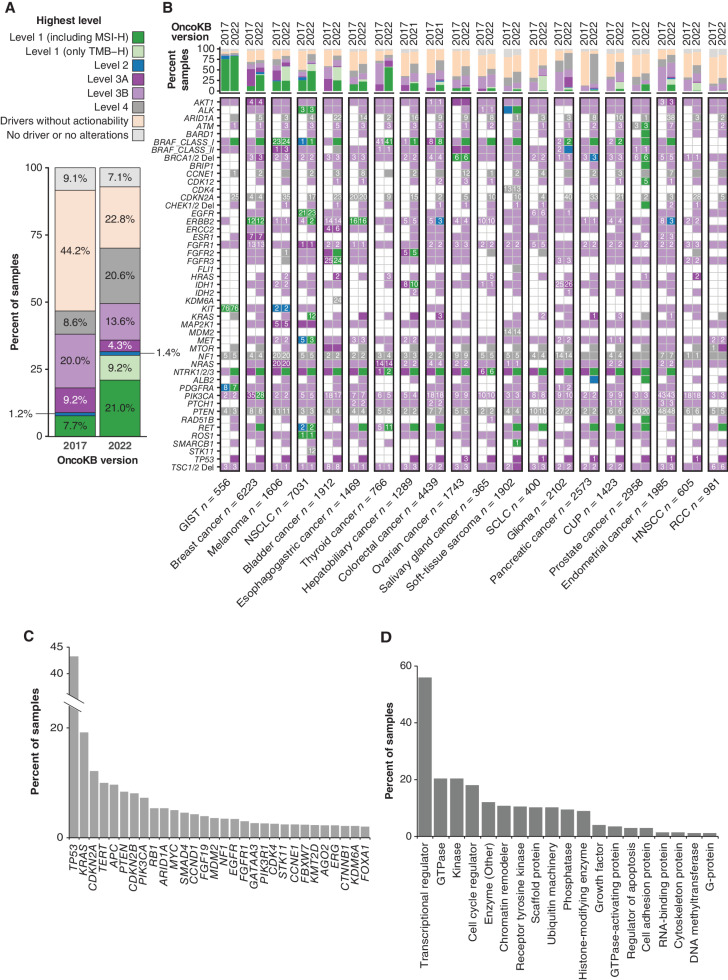
There is a continuing debate about the proportion of cancer patients that benefit from precision oncology, attributable in part to conflicting views as to which molecular alterations are clinically actionable. To quantify the expansion of clinical actionability since 2017, we annotated 47,271 solid tumors sequenced with the MSK-IMPACT clinical assay using two temporally distinct versions of the OncoKB knowledge base deployed 5 years apart. Between 2017 and 2022, we observed an increase from 8.9% to 31.6% in the fraction of tumors harboring a standard care (level 1 or 2) predictive biomarker of therapy response and an almost halving of tumors carrying nonactionable drivers (44.2% to 22.8%). In tumors with limited or no clinical actionability, TP53 (43.2%), KRAS (19.2%), and CDKN2A (12.2%) were the most frequently altered genes.
Significance: Although clear progress has been made in expanding the availability of precision oncology-based treatment paradigms, our results suggest a continued unmet need for innovative therapeutic strategies, particularly for cancers with currently undruggable oncogenic drivers. See related commentary by Horak and Fröhling, p. 18. This article is featured in Selected Articles from This Issue, p. 5.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
-
Measuring Progress in Precision Oncology.Cancer Discov. 2024 Jan 12;14(1):18-19. doi: 10.1158/2159-8290.CD-23-1237. Cancer Discov. 2024. PMID: 38213297
References
-
- Chakravarty D, Solit DB. Clinical cancer genomic profiling. Nat Rev Genet 2021;22:483–501. - PubMed
-
- Chakravarty D, Johnson A, Sklar J, Lindeman NI, Moore K, Ganesan S, et al. . Somatic genomic testing in patients with metastatic or advanced cancer: ASCO provisional clinical opinion. J Clin Oncol 2022;40:1231–58. - PubMed
-
- Ostrem JML, Shokat KM. Direct small-molecule inhibitors of KRAS: from structural insights to mechanism-based design. Nat Rev Drug Discov 2016;15:771–85. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
