

Segmenting computed tomograms for cardiac ablation using machine learning leveraged by domain knowledge encoding
- PMID: 37849936
- PMCID: PMC10577270
- DOI: 10.3389/fcvm.2023.1189293
Segmenting computed tomograms for cardiac ablation using machine learning leveraged by domain knowledge encoding
Abstract
Background: Segmentation of computed tomography (CT) is important for many clinical procedures including personalized cardiac ablation for the management of cardiac arrhythmias. While segmentation can be automated by machine learning (ML), it is limited by the need for large, labeled training data that may be difficult to obtain. We set out to combine ML of cardiac CT with domain knowledge, which reduces the need for large training datasets by encoding cardiac geometry, which we then tested in independent datasets and in a prospective study of atrial fibrillation (AF) ablation.
Methods: We mathematically represented atrial anatomy with simple geometric shapes and derived a model to parse cardiac structures in a small set of N = 6 digital hearts. The model, termed "virtual dissection," was used to train ML to segment cardiac CT in N = 20 patients, then tested in independent datasets and in a prospective study.
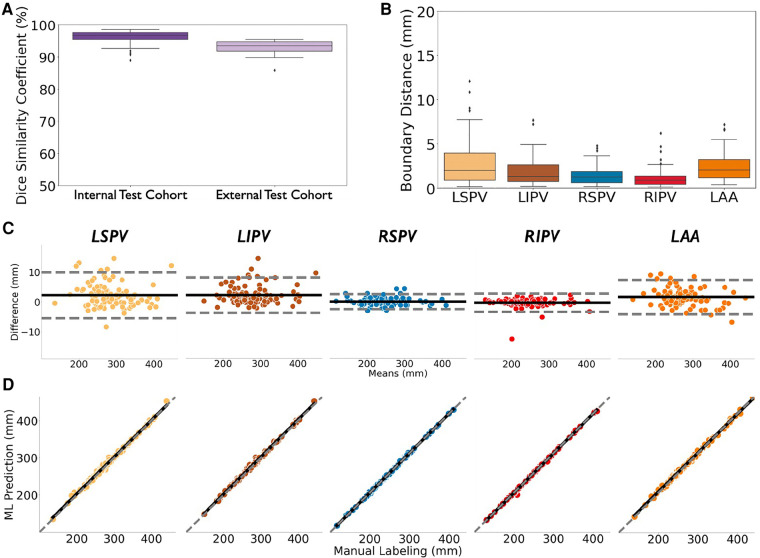
Results: In independent test cohorts (N = 160) from 2 Institutions with different CT scanners, atrial structures were accurately segmented with Dice scores of 96.7% in internal (IQR: 95.3%-97.7%) and 93.5% in external (IQR: 91.9%-94.7%) test data, with good agreement with experts (r = 0.99; p < 0.0001). In a prospective study of 42 patients at ablation, this approach reduced segmentation time by 85% (2.3 ± 0.8 vs. 15.0 ± 6.9 min, p < 0.0001), yet provided similar Dice scores to experts (93.9% (IQR: 93.0%-94.6%) vs. 94.4% (IQR: 92.8%-95.7%), p = NS).
Conclusions: Encoding cardiac geometry using mathematical models greatly accelerated training of ML to segment CT, reducing the need for large training sets while retaining accuracy in independent test data. Combining ML with domain knowledge may have broad applications.
Keywords: ablation; atrial fibrillation; cardiac CT segmentation; domain knowledge; machine learning; mathematical modeling.
© 2023 Feng, Deb, Ganesan, Tjong, Rogers, Ruipérez-Campillo, Somani, Clopton, Baykaner, Rodrigo, Zou, Haddad, Zahari and Narayan.
Conflict of interest statement
SN reports grant support from the National Institutes of Health (R01 HL149134 and R01 HL83359), consulting from Uptodate Inc., and TDK Inc., intellectual property owned by University of California Regents and Stanford University. FT: Consulting honoraria to institution from Abbott, Boston Scientific, Daiichi Sankyo; no personal gain. AR: grants from NIH (F32HL144101), NIH LRP, and Stanford SSPS. PC: consulting at American College of Cardiology. MR: equity interests in Corify Health Care. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- Narayan SM, Baykaner T, Clopton P, Schricker A, Lalani GG, Krummen DE, et al. Ablation of rotor and focal sources reduces late recurrence of atrial fibrillation compared with trigger ablation alone: extended follow-up of the confirm trial (conventional ablation for atrial fibrillation with or without focal impulse and rotor modulation). J Am Coll Cardiol. (2014) 63(17):1761–8. 10.1016/j.jacc.2014.02.543 - DOI - PMC - PubMed
-
- Biosense Webster I. Carto® 3 System Instructions for Use (V3.2.3) (2015). Available from: https://www.e-ifu.com/search-document-metadata/CARTO%C2%AE%203%20SYSTEM%...
-
- Zhu J, Liu Y, Zhang J, Wang Y, Chen L. Preliminary clinical study of the differences between interobserver evaluation and deep convolutional neural network-based segmentation of multiple organs at risk in Ct images of lung cancer. Front Oncol. (2019) 9:627. 10.3389/fonc.2019.00627. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous