

Cardiovascular Manifestations and Management in ADPKD
- PMID: 37850017
- PMCID: PMC10577330
- DOI: 10.1016/j.ekir.2023.07.017
Cardiovascular Manifestations and Management in ADPKD
Abstract
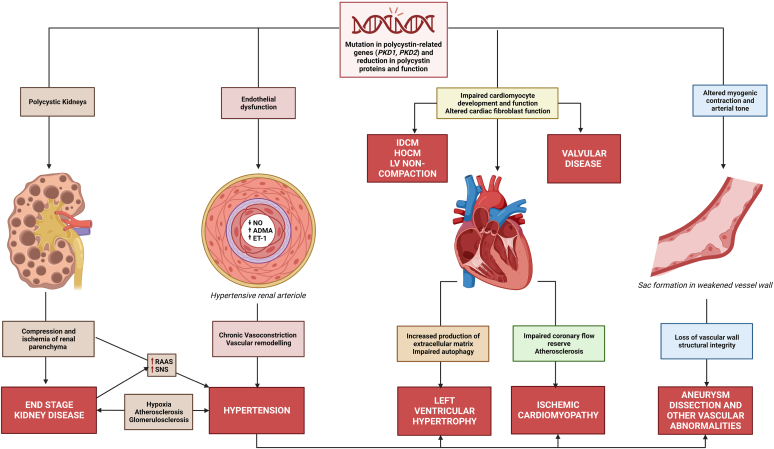
Cardiovascular disease (CVD) is the major cause of mortality in autosomal dominant polycystic kidney disease (ADPKD) and contributes to significant burden of disease. The manifestations are varied, including left ventricular hypertrophy (LVH), intracranial aneurysms (ICAs), valvular heart disease, and cardiomyopathies; however, the most common presentation and a major modifiable risk factor is hypertension. The aim of this review is to detail the complex pathogenesis of hypertension and other extrarenal cardiac and vascular conditions in ADPKD drawing on preclinical, clinical, and epidemiological evidence. The main drivers of disease are the renin-angiotensin-aldosterone system (RAAS) and polycystin-related endothelial cell dysfunction, with the sympathetic nervous system (SNS), nitric oxide (NO), endothelin-1 (ET-1), and asymmetric dimethylarginine (ADMA) likely playing key roles in different disease stages. The reported rates of some manifestations, such as LVH, have decreased likely due to the use of antihypertensive therapies; and others, such as ischemic cardiomyopathy, have been reported with increased prevalence likely due to longer survival and higher rates of chronic disease. ADPKD-specific screening and management guidelines exist for hypertension, LVH, and ICAs; and these are described in this review.
Keywords: autosomal dominant polycystic kidney disease; cardiovascular disease; endothelial dysfunction; hypertension; intracranial aneurysms; valvular heart disease.
Crown Copyright © 2023 Published by Elsevier Inc. on behalf of the International Society of Nephrology.
Figures
References
-
- Harris P.C., Torres V.E. Polycystic kidney disease, autosomal dominant. https://www.ncbi.nlm.nih.gov/books/NBK1246/
Publication types
LinkOut - more resources
Full Text Sources
