

Comparison of Balanced Crystalloids versus Normal Saline in Critically Ill Patients: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Trials
- PMID: 37850070
- PMCID: PMC10577264
- DOI: 10.2147/TCRM.S416785
Comparison of Balanced Crystalloids versus Normal Saline in Critically Ill Patients: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Trials
Abstract
Background: Fluid resuscitation is routinely needed for critically ill patients. However, the optimal choice between crystalloids and normal saline is in heat debate.
Objective: To conduct a meta-analysis comparing normal saline and balanced crystalloids in the treatment of critically ill patients with composite mortality as the primary outcome.
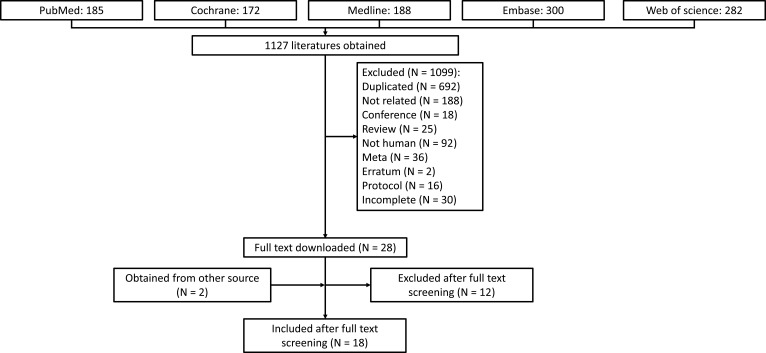
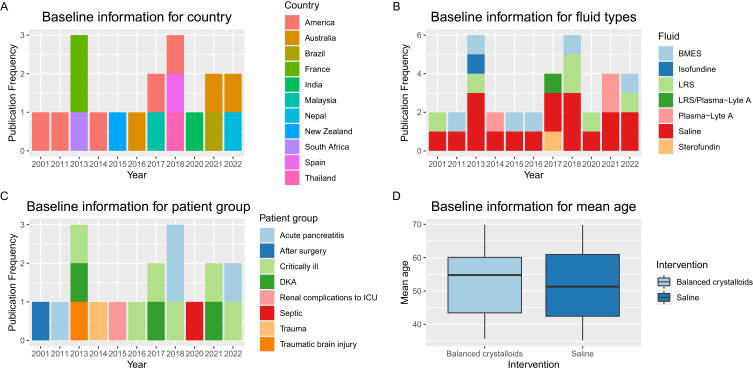
Methods: PubMed, Embase, Medline, Web of Science, and Cochrane Library were searched from inception up to March 2022. Studies of critically ill adult patients assigned to receive normal saline or balanced crystalloids were included. We conducted a meta-analysis using an inverse variance, random-effects model in addition to trial sequential analysis (TSA). The primary outcome was composite mortality. Subgroup analyses were also conducted.
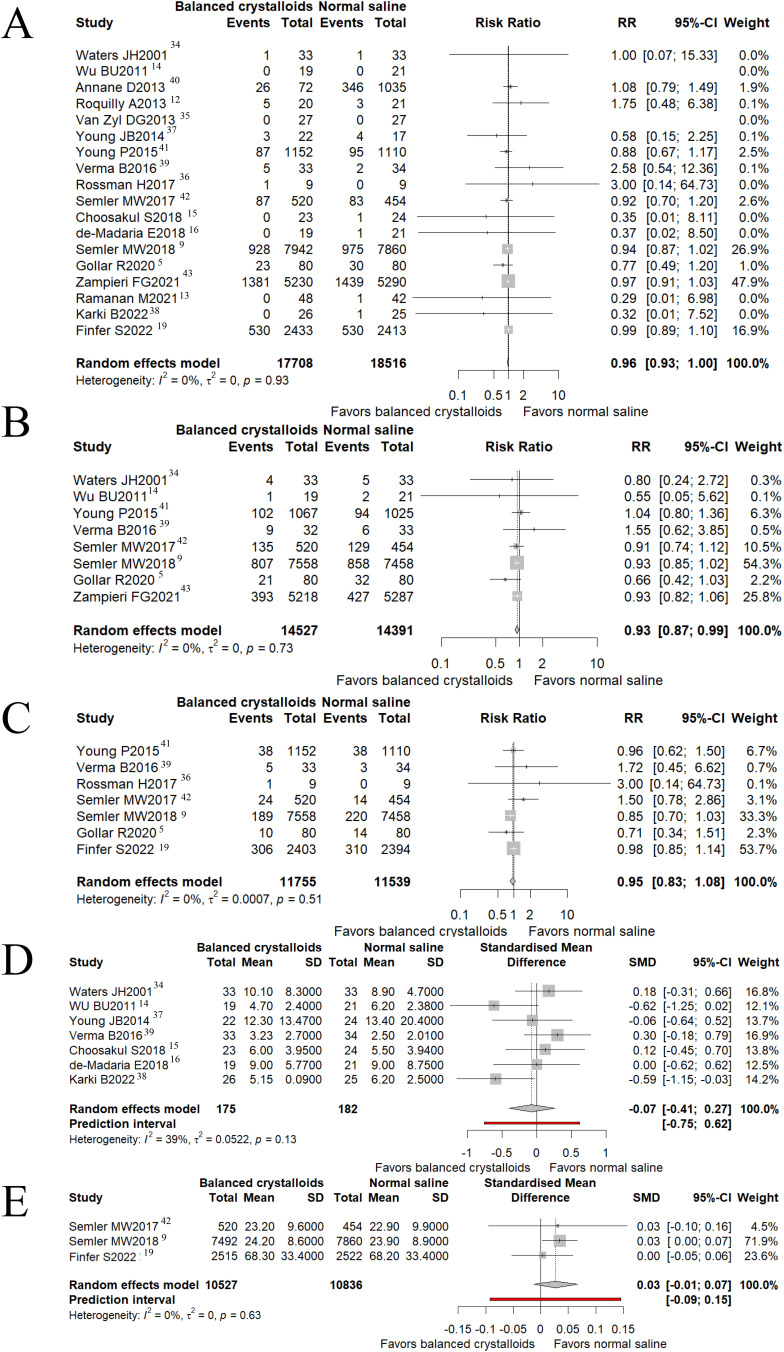
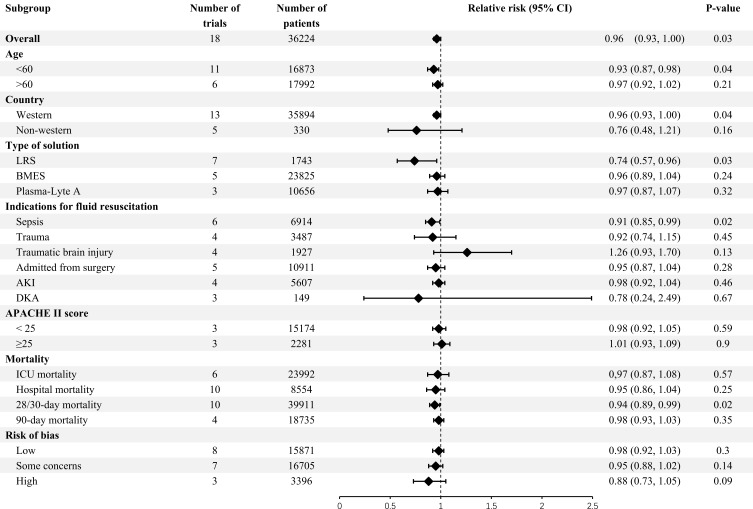
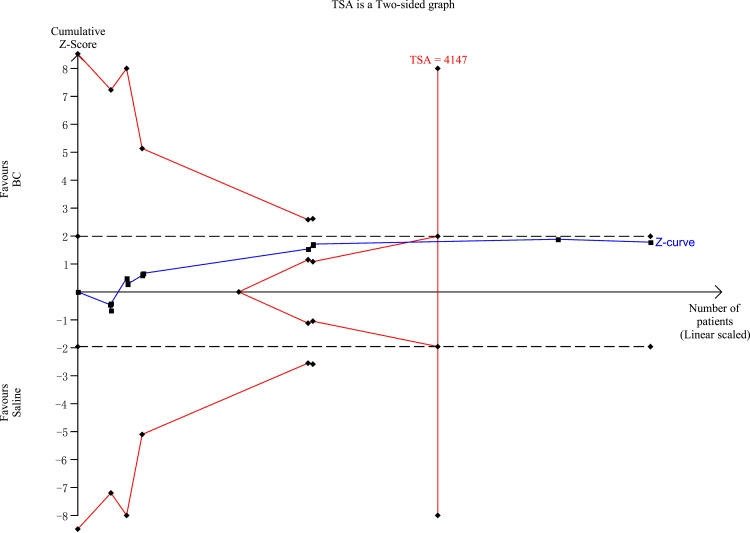
Results: Eighteen full-text studies (n=36,224) were included. Balanced crystalloids were associated with lower mortality compared with normal saline (risk ratio [RR]=0.96; 95% confidential interval [CI] 0.93, 1; p=0.03; I2=0) and lower incidence of acute kidney injury/acute renal failure (RR =0.93; 95% CI = 0.87, 0.99; p=0.03). No significant difference was observed in other outcomes. In the sepsis patients, the balanced crystalloid showed a lower composite mortality rate compared with normal saline (RR =0.91; 95% CI = 0.85, 0.99; p=0.02). TSA analysis demonstrated that, with 80% power, the effect of balanced crystalloid is not larger than a 10% relative decrease in composite mortality compared with normal saline.
Conclusion and relevance: This study demonstrated that balanced crystalloids could be an optimal choice over normal saline in critically ill patients to a reduced composite mortality rate. In patients with sepsis, the difference is especially significant. Nonetheless, the optimal resuscitation fluid option between saline and balanced crystalloid solutions should be investigated further with more evidence.
Keywords: balanced crystalloids; critically ill; meta-analysis; normal saline; systematic review.
© 2023 Chen and Gao.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Balanced crystalloids versus normal saline for fluid resuscitation in critically ill patients: A systematic review and meta-analysis with trial sequential analysis.Am J Emerg Med. 2019 Nov;37(11):2072-2078. doi: 10.1016/j.ajem.2019.02.045. Epub 2019 Mar 1. Am J Emerg Med. 2019. PMID: 30852043
-
Balanced Crystalloids Versus Saline in Critically Ill Adults: A Systematic Review and Meta-analysis.Ann Pharmacother. 2020 Jan;54(1):5-13. doi: 10.1177/1060028019866420. Epub 2019 Jul 31. Ann Pharmacother. 2020. PMID: 31364382
-
Fluid resuscitation with balanced crystalloids versus normal saline in critically ill patients: a systematic review and meta-analysis.Scand J Trauma Resusc Emerg Med. 2022 Apr 18;30(1):28. doi: 10.1186/s13049-022-01015-3. Scand J Trauma Resusc Emerg Med. 2022. PMID: 35436929 Free PMC article.
-
Balanced crystalloids versus saline in critically ill patients: The PRISMA study of a meta-analysis.Medicine (Baltimore). 2021 Sep 24;100(38):e27203. doi: 10.1097/MD.0000000000027203. Medicine (Baltimore). 2021. PMID: 34559108 Free PMC article.
-
Effects of chloride content of intravenous crystalloid solutions in critically ill adult patients: a meta-analysis with trial sequential analysis of randomized trials.Ann Intensive Care. 2019 Feb 13;9(1):30. doi: 10.1186/s13613-019-0506-y. Ann Intensive Care. 2019. PMID: 30758680 Free PMC article.
References
-
- Golla R, Kumar S, Dhibhar DP, Bhalla A, Sharma N. 0.9% saline V/S Ringer’s lactate for fluid resuscitation in adult sepsis patients in emergency medical services: an open-label randomized controlled trial. Hong Kong J Emerg Med. 2020;2020:1024907920948983. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
