

Two Years with a Tubeless Automated Insulin Delivery System: A Single-Arm Multicenter Trial in Children, Adolescents, and Adults with Type 1 Diabetes
- PMID: 37850941
- PMCID: PMC10794844
- DOI: 10.1089/dia.2023.0364
Two Years with a Tubeless Automated Insulin Delivery System: A Single-Arm Multicenter Trial in Children, Adolescents, and Adults with Type 1 Diabetes
Abstract
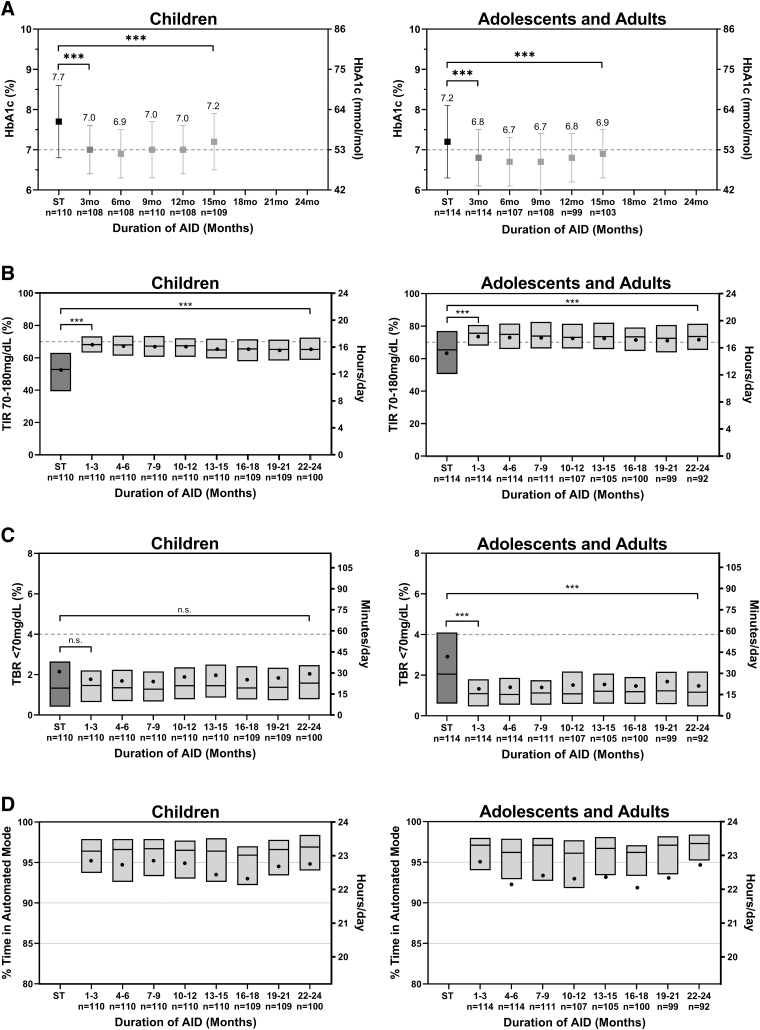
Background: The Omnipod® 5 Automated Insulin Delivery (AID) System was shown to be safe and effective following 3 months of use in people with type 1 diabetes (T1D); however, data on the durability of these results are limited. This study evaluated the long-term safety and effectiveness of Omnipod 5 use in people with T1D during up to 2 years of use. Materials and Methods: After a 3-month single-arm, multicenter, pivotal trial in children (6-13.9 years) and adolescents/adults (14-70 years), participants could continue system use in an extension phase. HbA1c was measured every 3 months for up to 15 months; continuous glucose monitor metrics were collected for up to 2 years. Results: Participants (N = 224) completed median (interquartile range) 22.3 (21.7, 22.7) months of AID. HbA1c was reduced in the pivotal trial from 7.7% ± 0.9% in children and 7.2% ± 0.9% in adolescents/adults to 7.0% ± 0.6% and 6.8% ± 0.7%, respectively, (P < 0.0001), and was maintained at 7.2% ± 0.7% and 6.9% ± 0.6% after 15 months (P < 0.0001 from baseline). Time in target range (70-180 mg/dL) increased from 52.4% ± 15.6% in children and 63.6% ± 16.5% in adolescents/adults at baseline to 67.9% ± 8.0% and 73.8% ± 10.8%, respectively, during the pivotal trial (P < 0.0001) and was maintained at 65.9% ± 8.9% and 72.9% ± 11.3% during the extension (P < 0.0001 from baseline). One episode of diabetic ketoacidosis and seven episodes of severe hypoglycemia occurred during the extension. Children and adolescents/adults spent median 96.1% and 96.3% of time in Automated Mode, respectively. Conclusion: Our study supports that long-term use of the Omnipod 5 AID System can safely maintain improvements in glycemic outcomes for up to 2 years of use in people with T1D. Clinical Trials Registration Number: NCT04196140.
Keywords: Artificial pancreas; Clinical trials; Closed-loop systems; Insulin pumps; Type 1 diabetes.
Conflict of interest statement
A.B.C. is an advisory board member of Insulet and has received grants and research support from Medtronic, Insulet, Dexcom, Abbott Diabetes, NIDDK, and grants from Sanofi and Lilly. A.L.C. is an advisory board member, has spoken for and received consulting fees from MannKind, Medtronic, and Sanofi; has received grants from Insulet, Dexcom, Medtronic, Abbott, Sanofi, Lilly, Novo Nordisk, UnitedHealth, and is an employee of the International Diabetes Center at Park Nicollet. S.A.B. reports research support to her institution from Insulet, Dexcom, Tandem Diabetes Care, Roche Diagnostics and Tolerion. G.P.F. has received consulting fees and grants from Insulet, Medtronic, Dexcom, Tandem, Lilly, and Beta Bionics, and grants from Abbott. B.W.B. has spoken for Lilly, Medtronic, Novo Nordisk, and Sanofi. B.W.B. has received research support from Insulet, Abbott, Advance, Diasome, Dexcom, Janssen, Lilly, Medtronic, Novo Nordisk, Provention Bio, Sanofi, Sanvita, Senseonics, REMD Biotherapeutics, Xeris, vTV Therapeutics, Boehringer Ingelheim, MannKind, and Zealand. C.J.L.'s is an advisory board member of Dexcom and has received grants from Dexcom and Abbott Diabetes. D.W.H. is employed by SUNY Upstate Medical University and has received grants from Insulet, Medtronic, and Boehringer Ingelheim. I.B.H. has received consulting fees from Abbott and Bigfoot and grants from Medtronic Diabetes, Insulet, and Beta Bionics. R.M.B reports research support, consulting, or service on a scientific advisory board for Abbott Diabetes Care, Ascensia, Bigfoot Biomedical, Dexcom, Hygieia, Eli Lilly, Medtronic, Novo Nordisk, Onduo, Roche, Sanofi, and United Health care and grants from the National Institutes of Health (NIH)/National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), and Helmsley Charitable Trust. R.M.B.'s employer, the nonprofit HealthPartners Institute, contracts for his services, and no personal income goes to him. J.L.S. is an advisory board member of Bigfoot Biomedical, Cecelia Health, Insulet, and Medtronic Diabetes. J.L.S. has received consulting fees from Cecelia Health, Eli Lilly, Lexicon, Insulet, Medtronic, and Sanofi and grants from Insulet, Medtronic, and NIDDK. S.N.M. has received grants from Insulet. L.M.L. has received consulting fees from Novo Nordisk, Lilly, Sanofi, Roche, Johnson & Johnson, Dexcom, Insulet, Boehringer Ingelheim, Convatec, Medtronic, Laxmi, Insulogic, and Lifescan, and grants from Insulet. V.N.S.'s employer, University of Colorado, reported receiving research support from NovoNordisk, Insulet, Tandem Diabetes care, Alexion, and Dexcom, an honoraria from Medscape, Lifescan, NovoNordisk, and DKSH Singapore for advisory board attendance, and from Insulet, Dexcom, Tandem Diabetes Care, and Embecta for speaking engagements. A.B. has received grants from AbbVie, Boehringer Ingelheim Pharma, Covance, Gan & Lee Pharma, Insulet, Janssen R&D, Lilly, Medtronic, Mylan N.V., Merck & Co, Tolerion, Novo Nordisk, Quintiles, Sanofi, Senseonics, Madrigal Pharma, Dexcom, Abbott, Viking, Poxel, Kowa Pharma America, and Boston Therapeutics. R.S.W. has received grants from Insulet, Lilly, Novo Nordisk, Tandem, Amgen, MannKind Corporation, Medtronic, Tolerion, Inc., Diasome Pharmaceuticals, Boehringer Ingelheim, and Kowa. S.A.M. is an advisory board member of Insulet. D.J.D. has received consulting fees from Dexcom and Insulet, and grants from Insulet. T.C.J. has received grants from Insulet. G.A. has received consulting fees from Bayer, Dexcom, Eli-Lilly, and Insulet; and grants from Dexcom, Inc., Eli-Lilly, Emmes, Fractyl Health, Insulet, Tandem Diabetes, and Welldoc. B.A.B. is an advisory board member of Convatec, Medtronic, and Tolerion. B.A.B. has received consulting fees from Insulet and Medtronic, and grants from Insulet, Medtronic, Tandem, Beta Bionics, Lilly, and NIDDK. T.T.L. is a full-time employee of and owns stock in Insulet Corporation. No other conflicts of interest were reported.
Figures
References
-
- American Diabetes Association Professional Practice C. 6. Glycemic targets: Standards of medical care in diabetes—2022. Diabetes Care 2021;45(Supplement_1):S83–S96. - PubMed
-
- Miller KM, Foster NC, Beck RW, et al. . Current state of type 1 diabetes treatment in the U.S.: Updated data from the T1D exchange clinic registry. Diabetes Care 2015;38(6):971–978. - PubMed
-
- Pettus JH, Zhou FL, Shepherd L, et al. . Incidences of severe hypoglycemia and diabetic ketoacidosis and prevalence of microvascular complications stratified by age and glycemic control in US adult patients with type 1 diabetes: A real-world study. Diabetes Care 2019;42(12):2220–2227. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical