

Uncovering heterogeneity in sepsis: a comparative analysis of subphenotypes
- PMID: 37851064
- PMCID: PMC10622359
- DOI: 10.1007/s00134-023-07239-w
Uncovering heterogeneity in sepsis: a comparative analysis of subphenotypes
Abstract
Purpose: The heterogeneity in sepsis is held responsible, in part, for the lack of precision treatment. Many attempts to identify subtypes of sepsis patients identify those with shared underlying biology or outcomes. To date, though, there has been limited effort to determine overlap across these previously identified subtypes. We aimed to determine the concordance of critically ill patients with sepsis classified by four previously described subtype strategies.
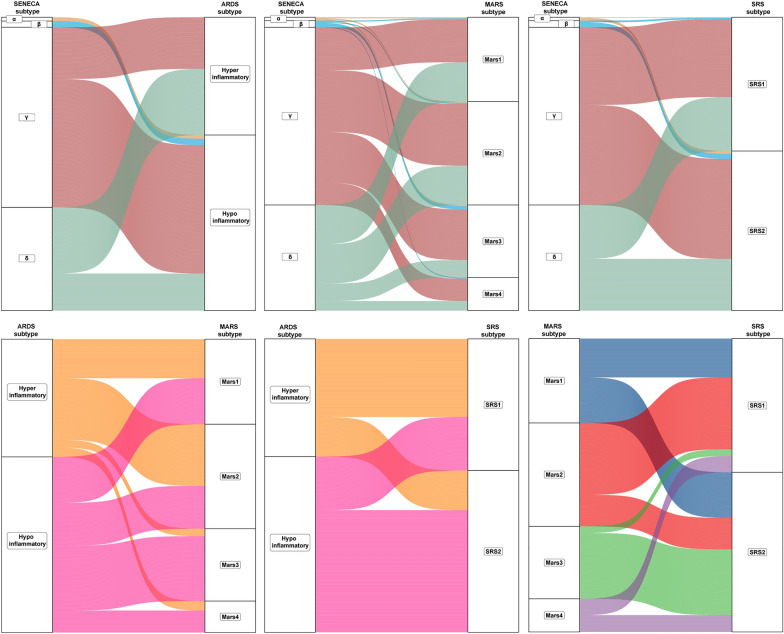
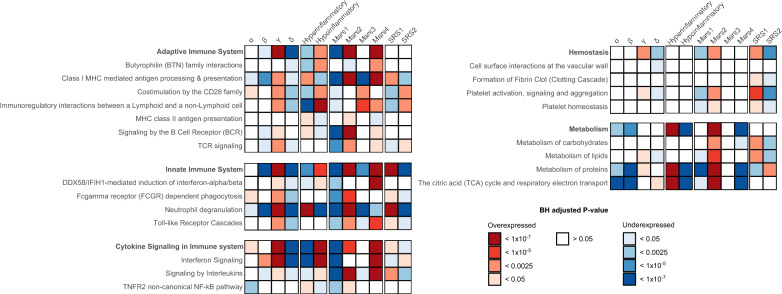
Methods: This secondary analysis of a multicenter prospective observational study included 522 critically ill patients with sepsis assigned to four previously established subtype strategies, primarily based on: (i) clinical data in the electronic health record (α, β, γ, and δ), (ii) biomarker data (hyper- and hypoinflammatory), and (iii-iv) transcriptomic data (Mars1-Mars4 and SRS1-SRS2). Concordance was studied between different subtype labels, clinical characteristics, biological host response aberrations, as well as combinations of subtypes by sepsis ensembles.
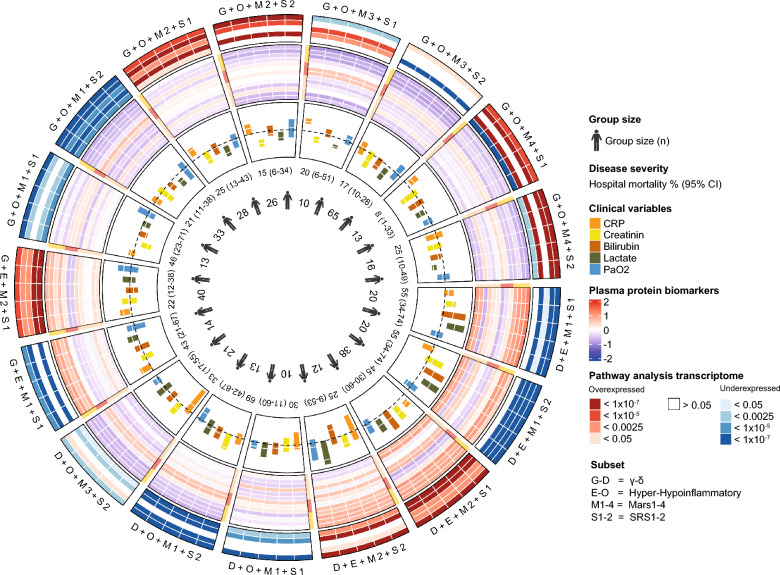
Results: All four subtype labels could be adjudicated in this cohort, with the distribution of the clinical subtype varying most from the original cohort. The most common subtypes in each of the four strategies were γ (61%), which is higher compared to the original classification, hypoinflammatory (60%), Mars2 (35%), and SRS2 (54%). There was no clear relationship between any of the subtyping approaches (Cramer's V = 0.086-0.456). Mars2 and SRS1 were most alike in terms of host response biomarkers (p = 0.079-0.424), while other subtype strategies showed no clear relationship. Patients enriched for multiple subtypes revealed that characteristics and outcomes differ dependent on the combination of subtypes made.
Conclusion: Among critically ill patients with sepsis, subtype strategies using clinical, biomarker, and transcriptomic data do not identify comparable patient populations and are likely to reflect disparate clinical characteristics and underlying biology.
Keywords: ARDS; Intensive care; Phenotype; Precision medicine; Sepsis.
© 2023. The Author(s).
Conflict of interest statement
The authors disclose that they do not have any potential conflicts of interest.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
