

Physiological effects of high-flow nasal cannula oxygen therapy after extubation: a randomized crossover study
- PMID: 37851284
- PMCID: PMC10584771
- DOI: 10.1186/s13613-023-01203-z
Physiological effects of high-flow nasal cannula oxygen therapy after extubation: a randomized crossover study
Abstract
Background: Prophylactic high-flow nasal cannula (HFNC) oxygen therapy can decrease the risk of extubation failure. It is frequently used in the postextubation phase alone or in combination with noninvasive ventilation. However, its physiological effects in this setting have not been thoroughly investigated. The aim of this study was to determine comprehensively the effects of HFNC applied after extubation on respiratory effort, diaphragm activity, gas exchange, ventilation distribution, and cardiovascular biomarkers.
Methods: This was a prospective randomized crossover physiological study in critically ill patients comparing 1 h of HFNC versus 1 h of standard oxygen after extubation. The main inclusion criteria were mechanical ventilation for at least 48 h due to acute respiratory failure, and extubation after a successful spontaneous breathing trial (SBT). We measured respiratory effort through esophageal/transdiaphragmatic pressures, and diaphragm electrical activity (ΔEAdi). Lung volumes and ventilation distribution were estimated by electrical impedance tomography. Arterial and central venous blood gases were analyzed, as well as cardiac stress biomarkers.
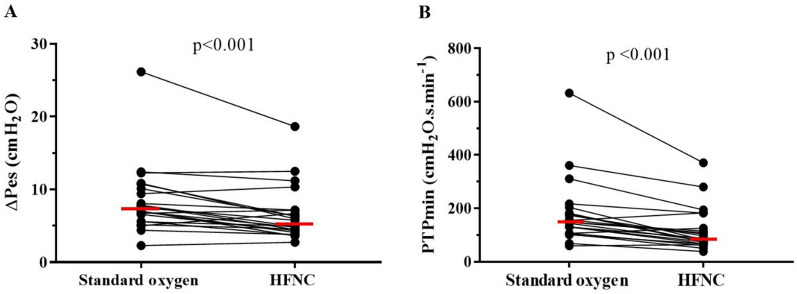
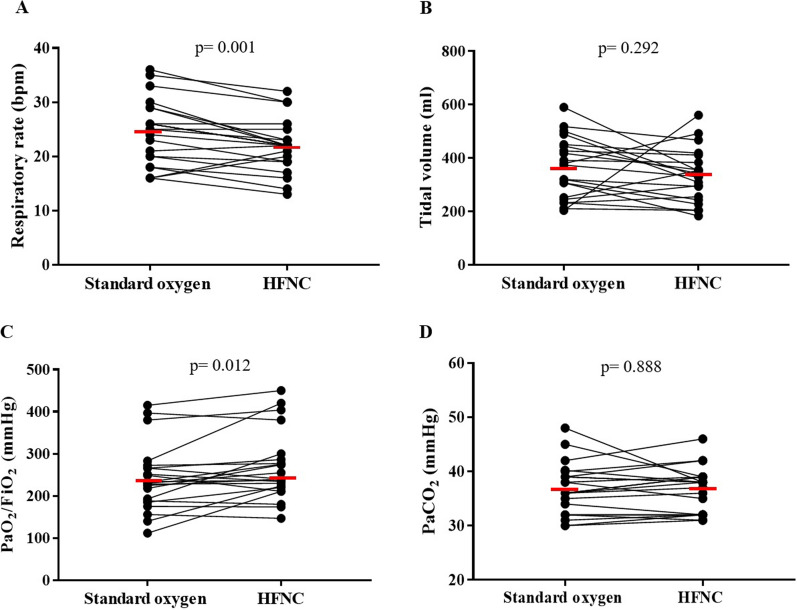
Results: We enrolled 22 patients (age 59 ± 17 years; 9 women) who had been intubated for 8 ± 6 days before extubation. Respiratory effort was significantly lower with HFNC than with standard oxygen therapy, as evidenced by esophageal pressure swings (5.3 [4.2-7.1] vs. 7.2 [5.6-10.3] cmH2O; p < 0.001), pressure-time product (85 [67-140] vs. 156 [114-238] cmH2O*s/min; p < 0.001) and ΔEAdi (10 [7-13] vs. 14 [9-16] µV; p = 0.022). In addition, HFNC induced increases in end-expiratory lung volume and PaO2/FiO2 ratio, decreases in respiratory rate and ventilatory ratio, while no changes were observed in systemic hemodynamics, Troponin T, or in amino-terminal pro-B-type natriuretic peptide.
Conclusions: Prophylactic application of HFNC after extubation provides substantial respiratory support and unloads respiratory muscles. Trial registration January 15, 2021. NCT04711759.
Keywords: Esophageal pressure; Reintubation; Weaning; Work of breathing.
© 2023. La Société de Réanimation de Langue Francaise = The French Society of Intensive Care (SRLF).
Conflict of interest statement
A.W.T has received speaking honoraria from Fisher and Paykel Healthcare.
Figures
Comment in
-
Letter on "Physiological effects of high-flow nasal cannula oxygen therapy after extubation: a randomized crossover study".Ann Intensive Care. 2024 Jan 11;14(1):8. doi: 10.1186/s13613-023-01234-6. Ann Intensive Care. 2024. PMID: 38206542 Free PMC article. No abstract available.
References
Associated data
Grants and funding
- Fondecyt 1191709/Agencia Nacional de Investigación y Desarrollo
- CONICYT-PFCHA/Doctorado Nacional 2020-folio 21201751/Agencia Nacional de Investigación y Desarrollo
- CONICYT-PFCHA/Doctorado Nacional 2019-folio 21191025/Agencia Nacional de Investigación y Desarrollo
- CONICYT-PFCHA/Doctorado Nacional 2021-folio 21212119/Agencia Nacional de Investigación y Desarrollo
LinkOut - more resources
Full Text Sources
Medical
