

Population Health Model Predicting the Long-Term Impact of Sotatercept on Morbidity and Mortality in Patients with Pulmonary Arterial Hypertension (PAH)
- PMID: 37851297
- PMCID: PMC10796519
- DOI: 10.1007/s12325-023-02684-x
Population Health Model Predicting the Long-Term Impact of Sotatercept on Morbidity and Mortality in Patients with Pulmonary Arterial Hypertension (PAH)
Abstract
Introduction: Pulmonary arterial hypertension (PAH) is a rare, progressive disease associated with significant morbidity and mortality. The phase 3 STELLAR trial tested sotatercept plus background therapy (BGT) versus placebo plus BGT. BGT was comprised of mono-, double-, or triple-PAH targeted therapy. Building on STELLAR findings, we employed a population health model to assess the potential long-term clinical impact of sotatercept.
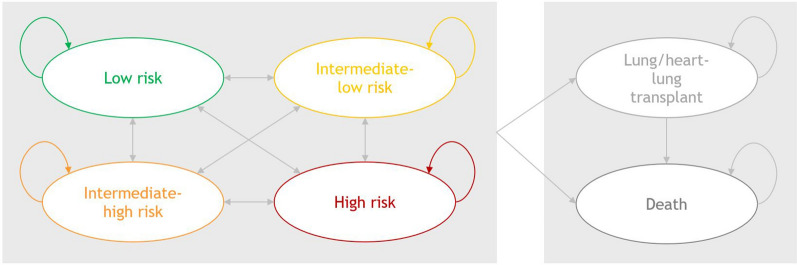
Methods: Based on the well-established ESC/ERS 4-strata risk assessment approach, we developed a six-state Markov-type model (low risk, intermediate-low risk, intermediate-high risk, high risk, lung/heart-lung transplant, and death) to compare the clinical outcomes of sotatercept plus BGT versus BGT alone over a lifetime horizon. State-transition probabilities were obtained from STELLAR. Risk stratum-adjusted mortality and lung/heart-lung transplant probabilities were based on COMPERA PAH registry data, and the post-transplant mortality probability was obtained from existing literature. Model outcomes were discounted at 3% annually. Sensitivity analyses were conducted to examine model robustness.
Results: In the base case, sotatercept plus BGT was associated with longer life expectancy from model baseline (16.5 vs 5.1 years) versus BGT alone, leading to 11.5 years gained per patient. Compared with BGT alone, sotatercept plus BGT was further associated with a gain in infused prostacyclin-free life years per patient, along with 683 PAH hospitalizations and 4 lung/heart-lung transplant avoided per 1000 patients.
Conclusions: According to this model, adding sotatercept to BGT increased life expectancy by roughly threefold among patients with PAH while reducing utilization of infused prostacyclin, PAH hospitalizations, and lung/heart-lung transplants. Real-world data are needed to confirm these findings.
Trial registration: ClinicalTrials.gov identifier, NCT04576988 (STELLAR).
Keywords: Pulmonary arterial hypertension; Risk strata; STELLAR; Sotatercept.
© 2023. Merck & Co., Inc., Rahway, NJ, USA and its affiliates.
Conflict of interest statement
Rongzhe Liu, Iman Nourhussein, and David Bernotas are employees (or were employees during conduct of this study) of OPEN Health, which received funding from Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA to conduct the study. Adnan Alsumali, Janethe de Oliveira Pena, Rogier Klok, Dominik Lautsch, Jestinah Chevure and Eliana Martinez are employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA and hold stock in Merck & Co., Inc., Rahway, NJ, USA. Vallerie McLaughlin is a consultant for Aerovate, Altavant Sciences, Bayer, CVS Caremark, CorVista Health, Gossamer Bio, Janssen, Merck, and United Therapeutics; and has received grants from Aerovate, Altavant Sciences, Merck, Gossamer Bio, Janssen, and SoniVie; and received stocks from Clene. Christine Pausch has nothing to disclose. Marius M. Hoeper is a consultant and speaker for Acceleron Pharma, Inc, Actelion, AOP Orphan Pharmaceuticals, Bayer, Ferrer, GlaxoSmithKline, Janssen, and MSD.
Figures

References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
