Psychotherapies for Generalized Anxiety Disorder in Adults: A Systematic Review and Network Meta-Analysis of Randomized Clinical Trials
- PMID: 37851421
- PMCID: PMC10585589
- DOI: 10.1001/jamapsychiatry.2023.3971
Psychotherapies for Generalized Anxiety Disorder in Adults: A Systematic Review and Network Meta-Analysis of Randomized Clinical Trials
Erratum in
-
Errors in Network Meta-Analysis.JAMA Psychiatry. 2024 Mar 1;81(3):320. doi: 10.1001/jamapsychiatry.2023.5480. JAMA Psychiatry. 2024. PMID: 38265778 Free PMC article. No abstract available.
-
Errors in Network Meta-Analysis of Generalized Anxiety Disorder Psychotherapies.JAMA Psychiatry. 2024 Mar 1;81(3):320. doi: 10.1001/jamapsychiatry.2023.5364. JAMA Psychiatry. 2024. PMID: 38265780 No abstract available.
Abstract
Importance: Generalized anxiety disorder (GAD) is one of the most common mental disorders in adults. Psychotherapies are among the most recommended treatments for GAD, but which should be considered as first-line treatment needs to be clarified.
Objective: To use a network meta-analysis to examine the short- and long-term associations of different psychotherapies with outcomes of effectiveness and acceptability in adults with GAD.
Data sources: MEDLINE, Embase, PsycINFO, and the Cochrane Register of Controlled Trials were searched from database inception to January 1, 2023, to identify randomized clinical trials (RCTs) of psychotherapies for adults with GAD.
Study selection: RCTs comparing any type of psychotherapy against another or with a control condition for the treatment of adults (≥18 years, both sexes) with a primary diagnosis of GAD were eligible for inclusion.
Data extraction and synthesis: This study followed Cochrane standards for extracting data and assessing data quality and used the PRISMA guideline for reporting. Risk of bias of individual studies was assessed using the second version of the Cochrane risk of bias tool, and the Confidence in Network Meta-Analysis was used to rate the certainty of evidence for meta-analytical results.
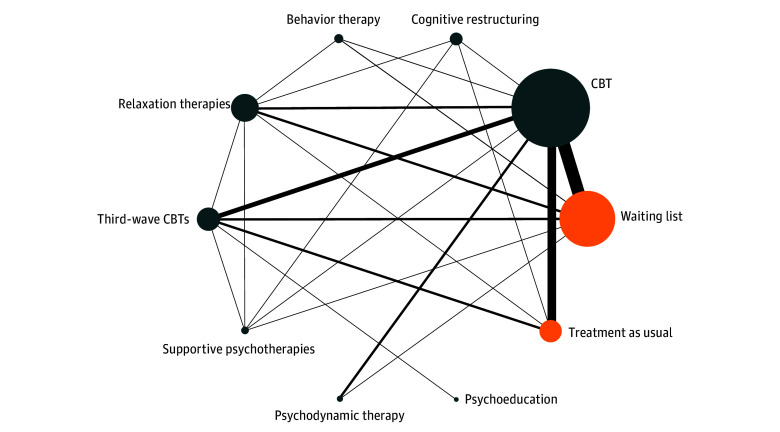
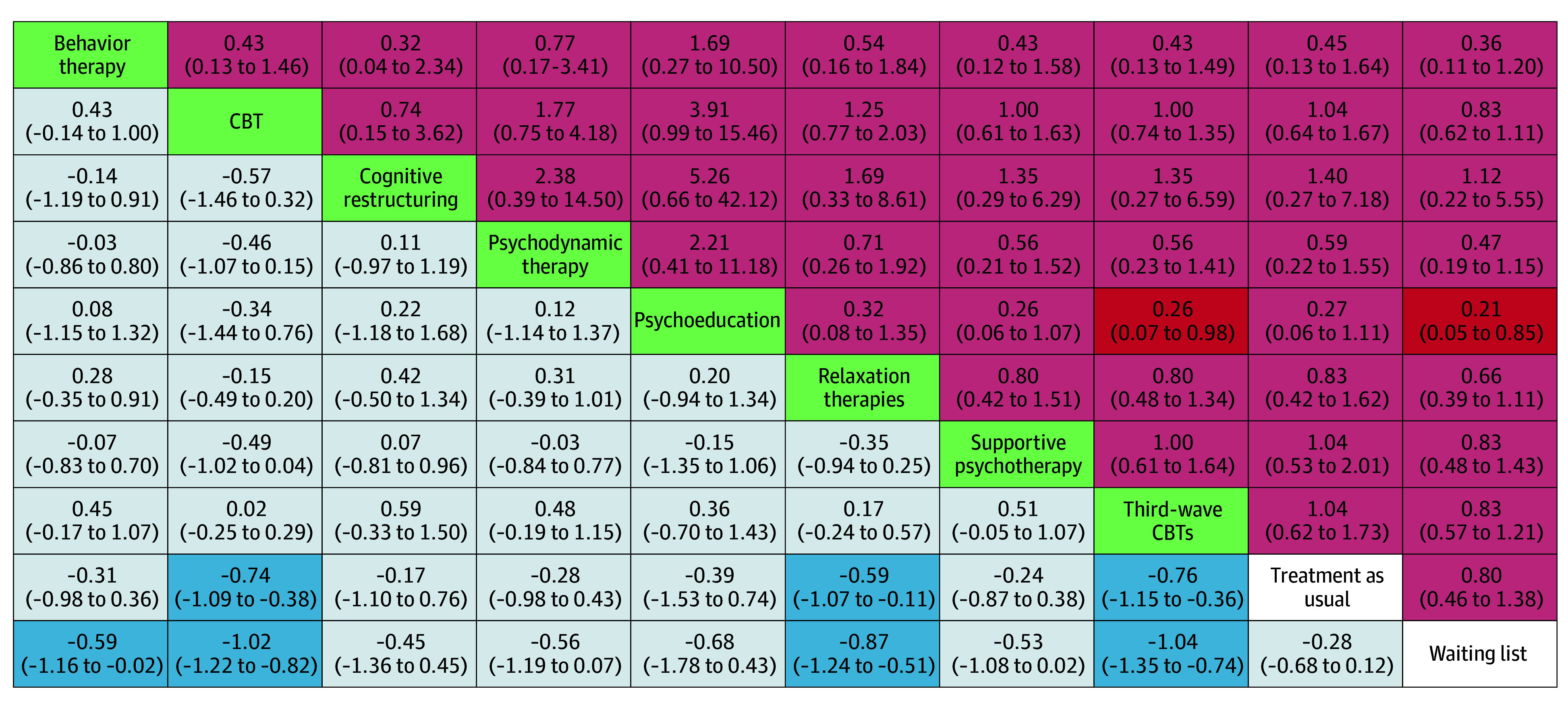
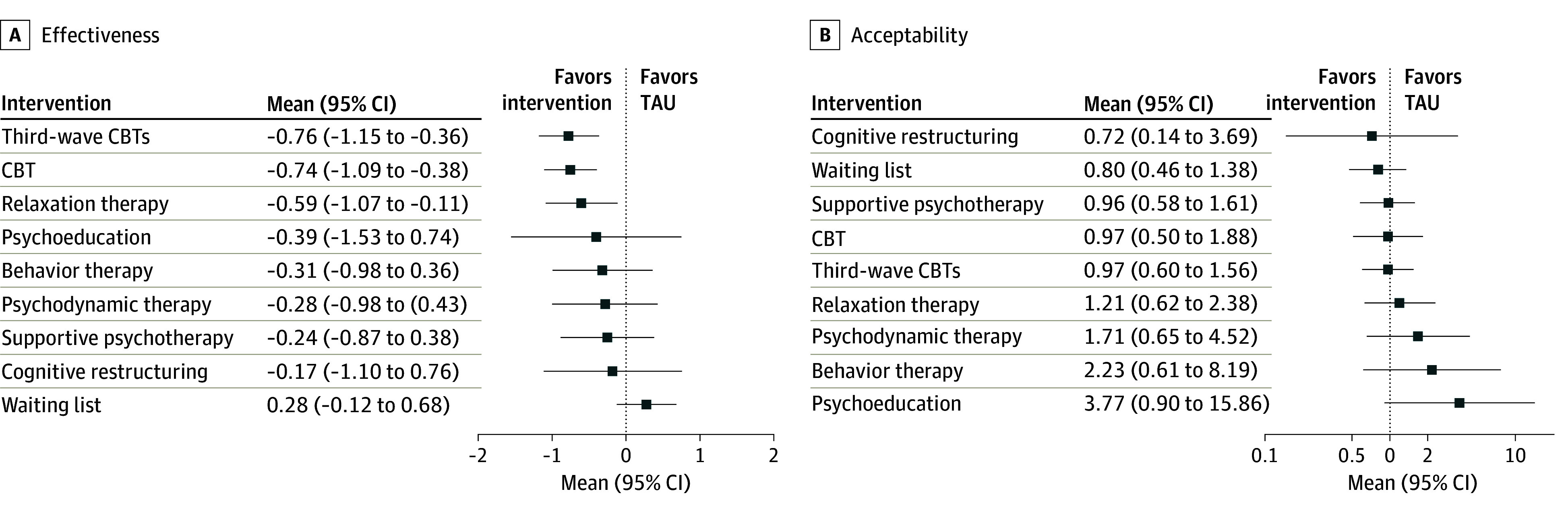
Main outcomes and measures: Eight psychotherapies were compared against one another and with 2 control conditions. Primary outcomes were severity of GAD symptoms and acceptability of the psychotherapies. Random-effects model pairwise and network meta-analyses were conducted. For effectiveness, standardized mean differences (SMDs) were pooled, and for acceptability, relative risks with 95% CIs were calculated.
Results: Data from 65 RCTs were included. Effect size estimates on data from 5048 participants (mean [SD], 70.9% [11.9%] women; mean [SD] age, 42.2 [12.5] years) suggested that third-wave cognitive behavior therapies (CBTs) (SMD, -0.76 [95% CI, -1.15 to -0.36]; certainty, moderate), CBT (SMD, -0.74 [95% CI, -1.09 to -0.38]; certainty, moderate), and relaxation therapy (SMD, -0.59 [95% CI, -1.07 to -0.11]; certainty, low) were associated with reduced GAD symptoms vs treatment as usual. Relative risks for all-cause discontinuation (indication of acceptability) signaled no differences compared with treatment as usual for all psychotherapies (eg, relative risk, 1.04 [95% CI, 0.64-1.67] for CBT vs treatment as usual). When excluding studies at high risk of bias, relaxation therapy lost its superiority over treatment as usual (SMD, -0.47; 95% CI, -1.18 to 0.23). When considering anxiety severity at 3 to 12 months after completion of the intervention, only CBT remained significantly associated with greater effectiveness than treatment as usual (SMD, -0.60; 95% CI, -0.99 to -0.21).
Conclusions and relevance: Given the evidence in this systematic review and network meta-analysis for its associations with both acute and long-term effectiveness, CBT may represent the first-line therapy of GAD. Third-wave CBTs and relaxation therapy were associated with short-term effectiveness and may also be offered.
Conflict of interest statement
Figures